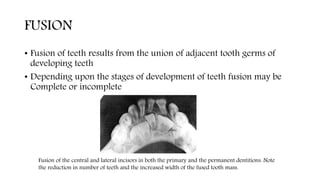
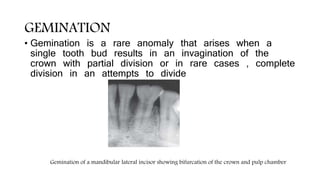
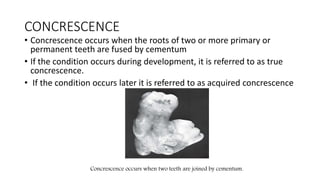
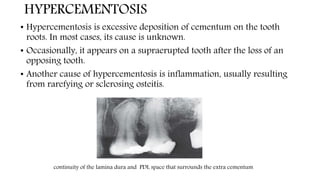
This document discusses the radiographic interpretation of various dental anomalies and implants. It provides examples of different dental anomalies like supernumerary teeth, macrodontia, microdontia, fusion, gemination, concrescence, hypercementosis, taurodontism, and dilaceration among others. It also discusses radiographic interpretations related to systemic conditions, presurgical implant imaging, post-implant imaging, and the classification of peri-implant radiolucencies. The goal of radiographic interpretation is to identify disease, understand its nature and extent, and assist in differential diagnosis.