Maxillary sinus
•Download as PPTX, PDF•
33 likes•10,061 views

These are the presentation prepared by student of BPKIHS Batch 2015 BDS on observation of respective faculty of BPKIHS

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Maxillary sinus
Similar to Maxillary sinus (20)
More from Amrit Jaishi
Recently uploaded
Recently uploaded (20)
Maxillary sinus
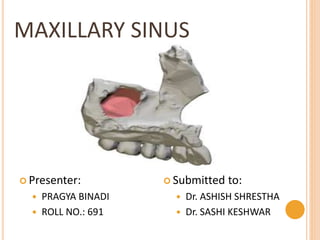
- 1. MAXILLARY SINUS Presenter: PRAGYA BINADI ROLL NO.: 691 Submitted to: Dr. ASHISH SHRESTHA Dr. SASHI KESHWAR
- 3. PARANASAL SINUSES Paranasal sinuses are air-filled spaces present within some bones around the nasal cavities. There are four pairs of paranasal sinuses: Maxillary Frontal Ethmoidal Sphenoidal All of the sinuses open into nasal cavity through its lateral wall.
- 5. DEFINATION Maxillary sinus is the pneumatic space that is lodged inside the body of maxilla and that communicates with the environment by way of the middle meatus and the nasal vestibule. Largest paranasal sinus Also called as “ANTRUM OF HIGHMORE” Drains into nose through Ostia.
- 7. ANATOMY Shape: Pyramidal Size: Variable Boundaries Apex: Zygomatic process of maxilla Base: Nasal surface of maxilla(formed by lateral wall of nose) Roof: Orbital surface of maxilla(formed by thin orbital part) Floor: Lateral hard palate, Alveolar process of maxilla Anterior wall is related to infra-orbital plexus of nerves and vessels and origin of muscles of upper lip Posterior wall is pierced by posterior superior alveolar nerve and vessels which travel to molar teeth.
- 9. BLOOD SUPPLY Arterial supply Facial artery Maxillary artery Infra orbital artery Greater palatine artery Venous drainage Anteriorly: Sphenopalatine vein Posteriorly: Pterygoid venous plexus drain into facial vein Pterygoid plexus communicates with cavernous sinus by emissary vein.
- 10. BLOOD SUPPLY
- 11. Nerve supply Anterior superior alveolar nerve Middle superior alveolar nerve Posterior superior alveolar nerve Infra orbital nerve Greater palatine Lymphatic drainage Submandibular lymph node Deep cervical lymph node Retropharyngeal lymph node
- 13. DEVELOPMENT It is the first paranasal sinus to develop. Initial development of sinus follows a number of morphogenic events in the differentiation of the nasal cavity in early gestation(about 32 mm crown-rump length [CRL] in an embryo.) Horizontal shift of the Palatal Shelves & subsequent fusion with one another
- 14. Nasal Septum separates the secondary oral cavity from the two nasal chambers Influences further expansion of the lateral nasal wall & 3 walls begin to fold 3 conchae and meatuses arise Superior and inferior meatuses remain as shallow depressions along the lateral nasal wall for the first half of IUL Middle meatus expands immediately into lateral nasal wall & expands in an inferior direction occupying more of the future maxillary body
- 15. Development of sinus starts at 12th week as an evagination of the mucous membrane in the lateral wall of the middle meatus In its development : Tubular at birth Ovoid at childhood Pyramidal in adulthood
- 16. MICROSCOPIC FEATURES Three layers surround the space of the Maxillary sinus: 1. Epithelial Layer 2. Basal Lamina 3. Sub – epithelial layer including periosteum Lined by pseudostratified columnar epithelium Columnar ciliated cells are numerous Additional cells: Basal cells, Columnar non ciliated cells, Goblet cells
- 17. Cilia contains 9+1 pairs of microtubules Cilia spreads the mucus Goblet cells are flask shaped cells, present in the basal layer, secrete mucus Sub epithelial glands provide serous and mucous secretion to the sinus
- 19. FUNCTION 1. Imparts resonance to the voice 2. Increases the surface area and lightens the skull 3. Moistens and warms inspired air 4. Filters the debris from the inspired air 5. Mucus production and storage 6. Limit extent of facial injury from trauma 7. Provides thermal insulation to important tissues 8. Serves as accessory olfactory organs
- 20. CLINICAL IMPORTANCE Dental infection: Infection from the maxillary premolar and molars can easily communicate and infect the maxillary antrum Oroantral Communication: Traumatic extraction of maxillary teeth can cause oroantral communication Root Pieces: Root pieces of maxillary teeth may sometimes be accidentally forced into the maxillary antrum Maxillary sinusitis: Because of the thickened and inflamed sinus lining compresses the nerve supply of the maxillary posterior teeth causing tenderness of the maxillary teeth the infraorbital and superior alveolar vessels are frequently ruptures in maxillary fracture causing the hematoma formation in the antrum.
- 21. CLINICAL CONSIDERATION 1. Maxillary sinusitis: It is the inflammation of the maxillary sinus mucosa. Types : Depending upon duration a. Acute (< 4 weeks) b. Sub acute (4 – 12 weeks) c. Chronic (going on for 12 weeks or more) Can sinusitis cause dental pain? One of the common symptoms of sinusitis is pain and the location depends on which sinus is affected. If pain is in patients upper jaw and teeth ,with tender cheeks, may mean the patients maxillary sinus is involved.
- 22. 1. Oroantral fistula It is an abnormal condition where the maxillary sinus is exposed to oral cavity through an epithelialised fistula. Oroantral communication(abnormal communication between maxillary sinus and oral cavity) if left untreated can either heal or progress into OAF. Causes of OAF Extraction of posterior maxillary molars mainly 1st and 2nd Displacement of posterior maxillary molar roots into antrum(palatal root mainly involved)
- 23. DEVELOPMENTAL ANOMALIES Crouzon syndrome: Early synostosis(fusion)of sutures produces hypoplasia of the maxilla and therefore the maxillary sinus together with the high arched palate. It is a genetic disorder charactarized by premature fusion of certain skull bones. Treacher Collins syndrome: Associated with grossly and symmetrically underdeveloped maxillary sinuses and malar bones. Binder syndrome: Hypoplasia of middle third of the face with smaller maxillary length and maxillary sinus hypoplasia.
- 24. REFERENCES B D CHAURASIA’S HUMAN ANATOMY ORBANS ORAL HISTOLOGY AND EMBRYOLOGY JAMES K AVERY ESSENTIALS OF ORAL HISTOLOGY AND EMBRYOLOGY