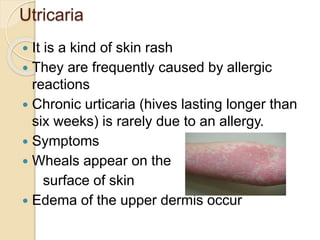
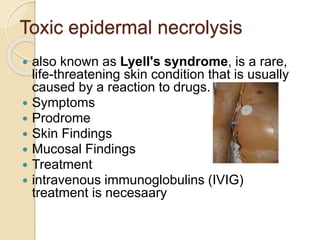
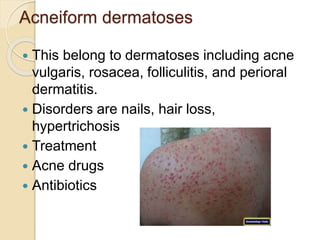
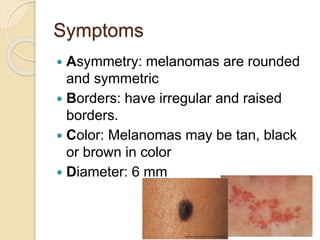
This document discusses dermal toxicology and cutaneous toxicity. It covers the anatomy of the skin, factors that affect absorption of toxicants through the skin like hydration and damage. It also outlines various conditions that can manifest from dermal exposure like contact dermatitis, ulcers, urticaria, toxic epidermal necrolysis, acneiform dermatoses, pigment disturbances, and skin cancer. Treatment options are provided for some of these conditions. Additionally, some toxicants present in foods that can cause dermal diseases are listed.
























































![Special dermalogiacl therapyies [final]](https://cdn.slidesharecdn.com/ss_thumbnails/specialdermalogiacltherapyiesfinal-200717060942-thumbnail.jpg?width=640&height=640&fit=bounds)



















![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)














