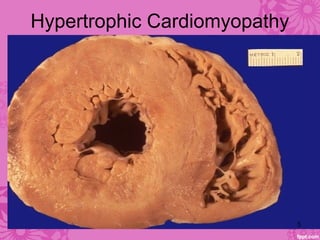
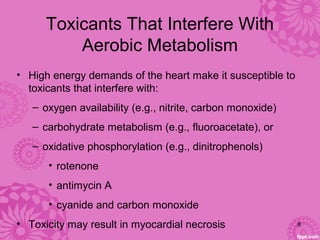
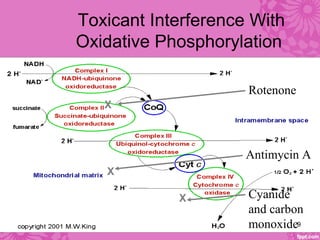
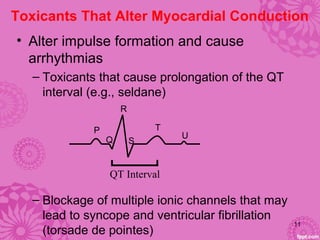
Cardiotoxicity refers to heart damage caused by certain chemotherapy drugs, heavy metals, and other toxins. Three main mechanisms of cardiotoxicity are discussed: interfering with aerobic metabolism in the heart, altering myocardial conduction, and directly damaging heart muscle cells. Symptoms of cardiotoxicity include fatigue, shortness of breath, and swelling. Diagnosis involves physical exams, imaging tests like echocardiograms and MUGA scans, and blood tests. Prevention strategies center around modifying drug treatment plans, using protective medications like dexrazoxane, and controlling risk factors after treatment through medications like ACE inhibitors and beta-blockers.