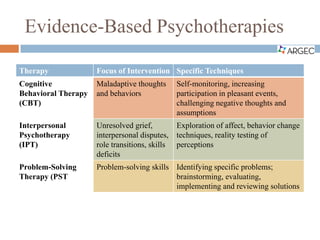
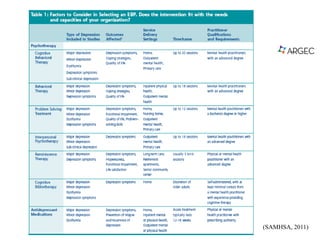
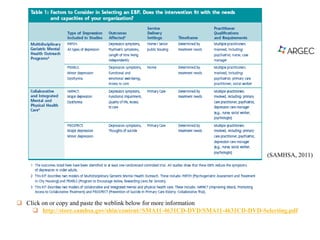
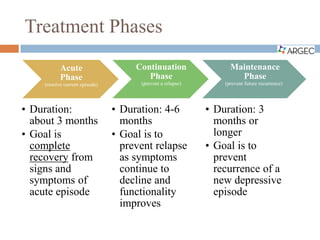
This document discusses depression in older adults, including barriers to treatment, treatment goals and modalities, and considerations for providers and patients. It describes common psychotherapies and pharmacotherapies used to treat depression at different phases. The goals are to resolve current episodes, prevent relapse and recurrence, and improve quality of life and functioning. Barriers include inadequate treatment, lack of accessible care, and limited specialty mental health use.