This document provides information on geriatric psychiatry and aging-related mental health issues. It discusses several key topics:
1. Age-related changes in physiological functioning can increase vulnerability over time. Late adulthood begins around age 65 and is characterized by gradual decline in functioning of body systems.
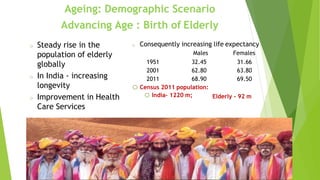
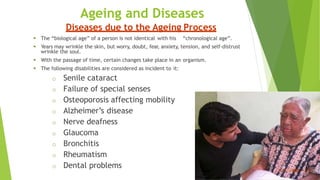
2. Life expectancy has been increasing in India and globally, leading to growth in the elderly population. Common concerns for elderly include retirement, economic insecurity, declining health, and loss of independence.
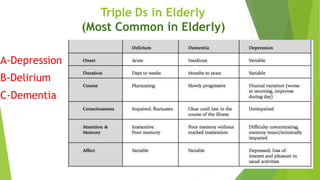
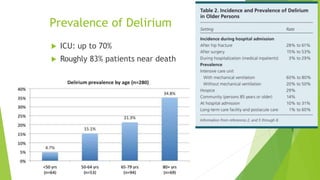
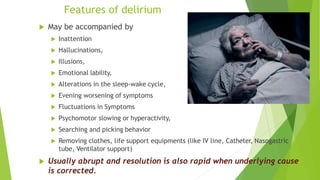
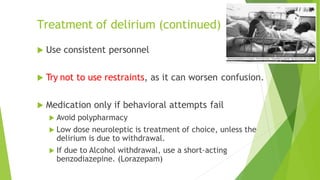
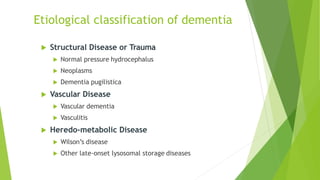
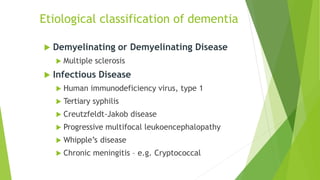
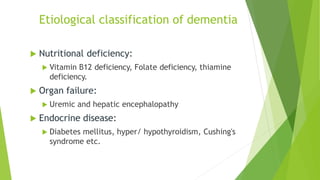
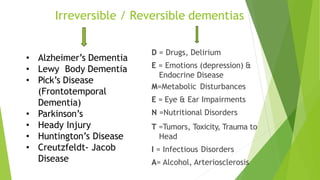
3. Major mental health disorders in elderly include depression, delirium, and dementia. Late-life depression can present differently than depression in younger populations. Delirium is an acute change in mental status that commonly affects hospital


































![Somatic Symptom and Related Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ssrdv1-200526002841-thumbnail.jpg?width=640&height=640&fit=bounds)











































