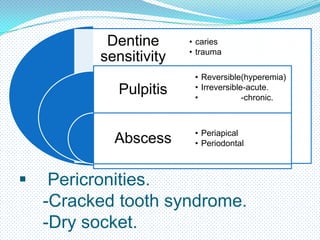
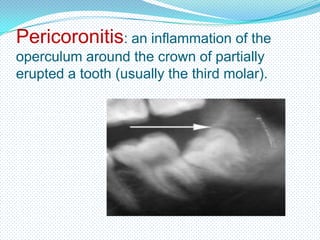
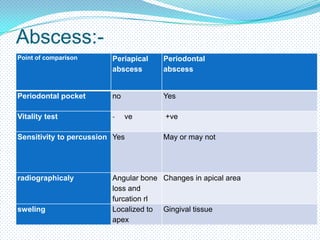
This document provides information on assessing and diagnosing various types of orofacial pain, including dental pain, dentine sensitivity, pulpitis, abscess, pericoronitis, dry socket, trigeminal neuralgia, preherpetic neuralgia, and atypical odontalgia. It describes the nature, symptoms, causes, diagnosis, and management of each condition. Key factors assessed include the location, duration, and triggers of the pain, as well as relevant medical and dental history. Diagnosis involves clinical examination, vitality testing, percussion, and radiography to determine the specific cause and appropriate treatment.



























































![Presentation1 [Autosaved].pdf diagnosiss](https://cdn.slidesharecdn.com/ss_thumbnails/presentation1autosaved-250812162634-6365894a-thumbnail.jpg?width=640&height=640&fit=bounds)





























