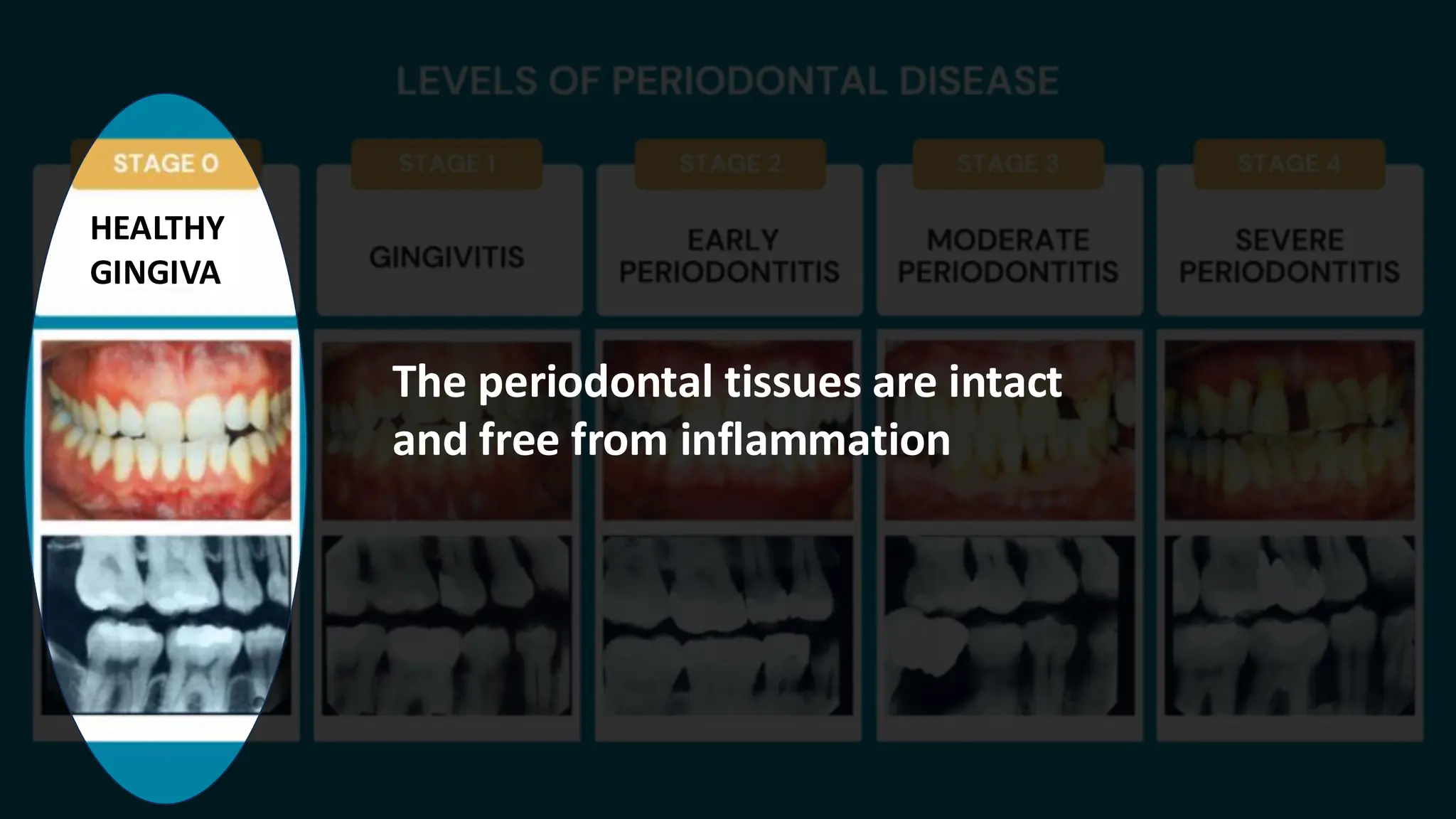
HEALTHY
GINGIVA
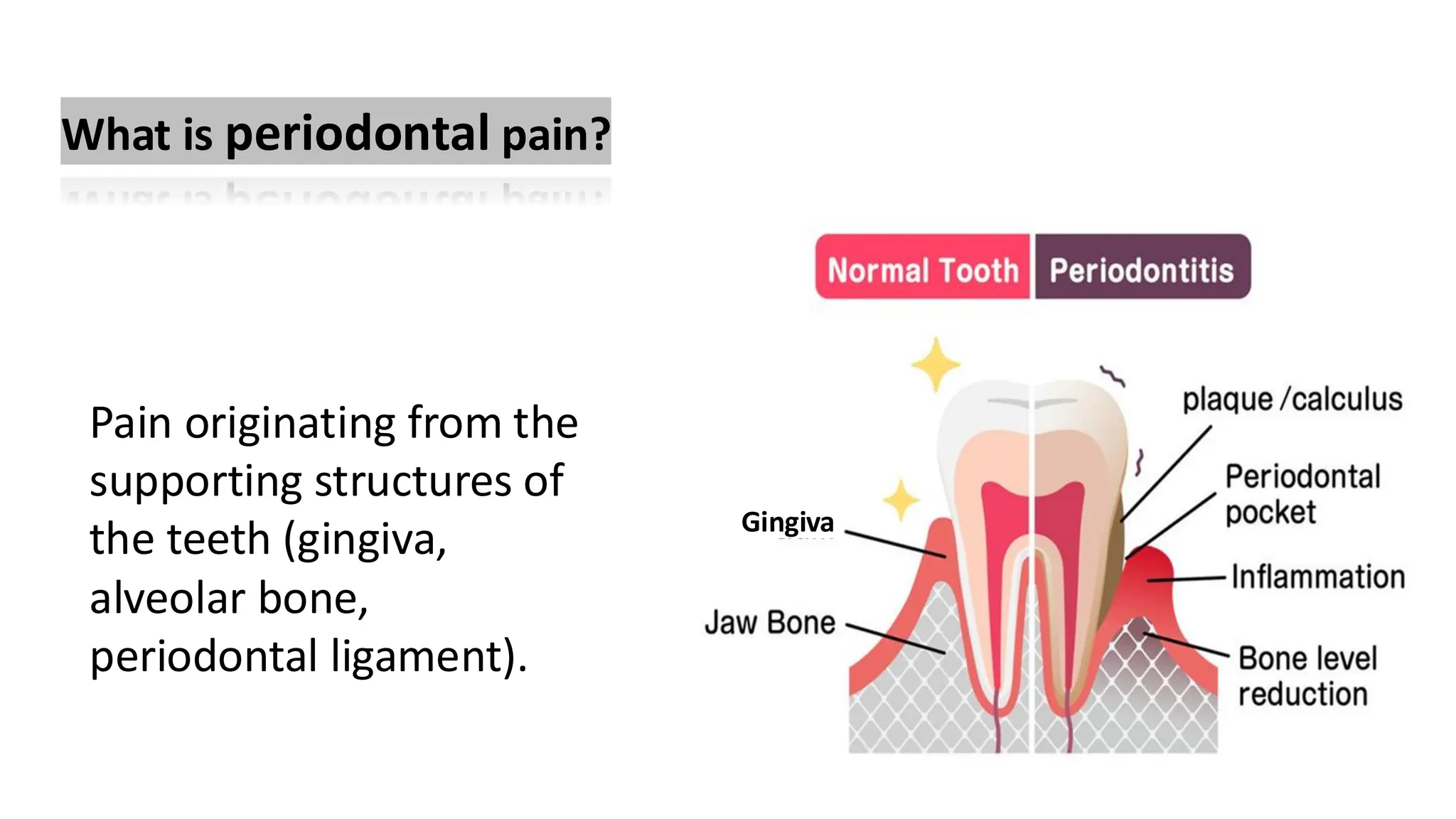
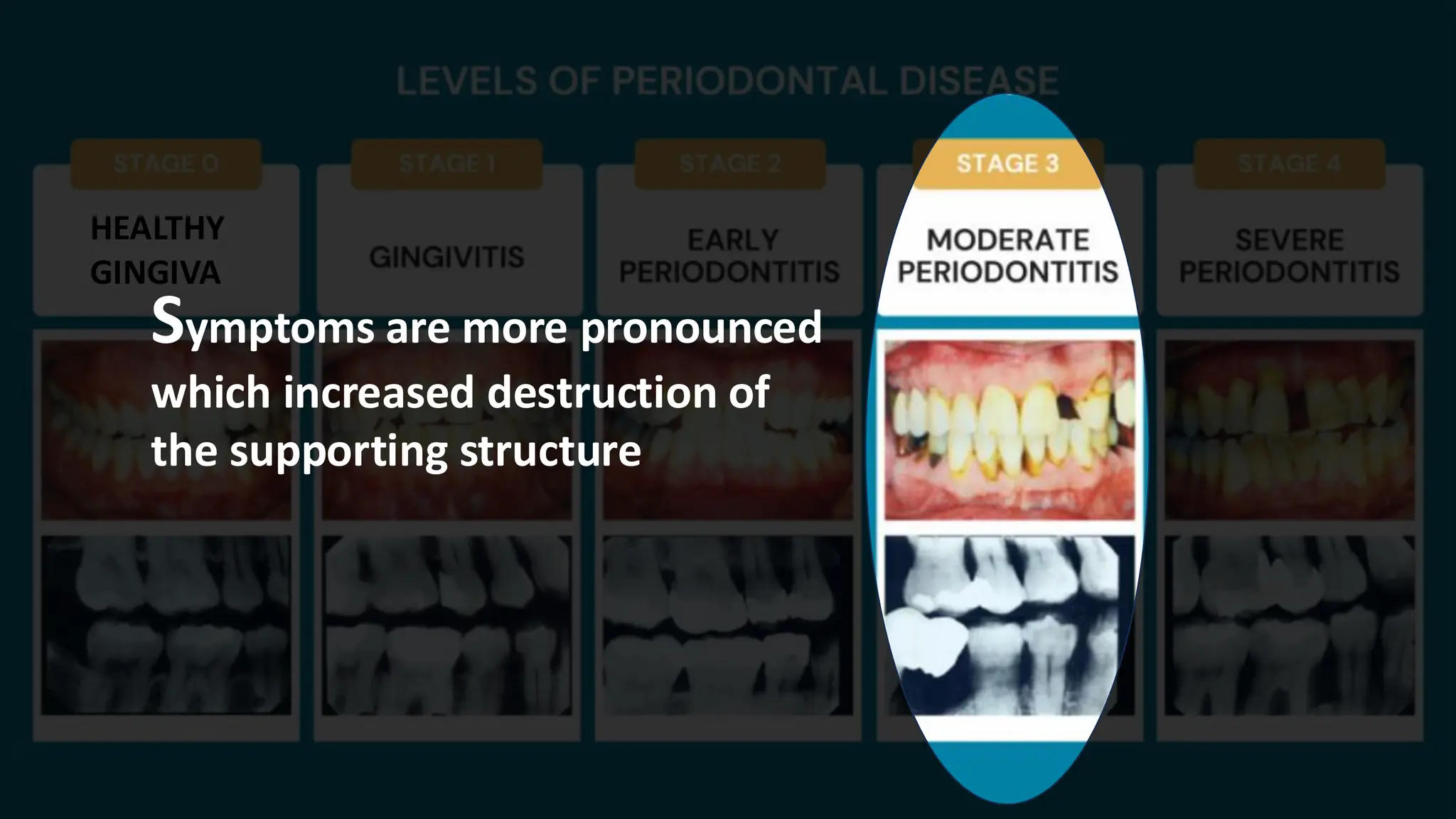
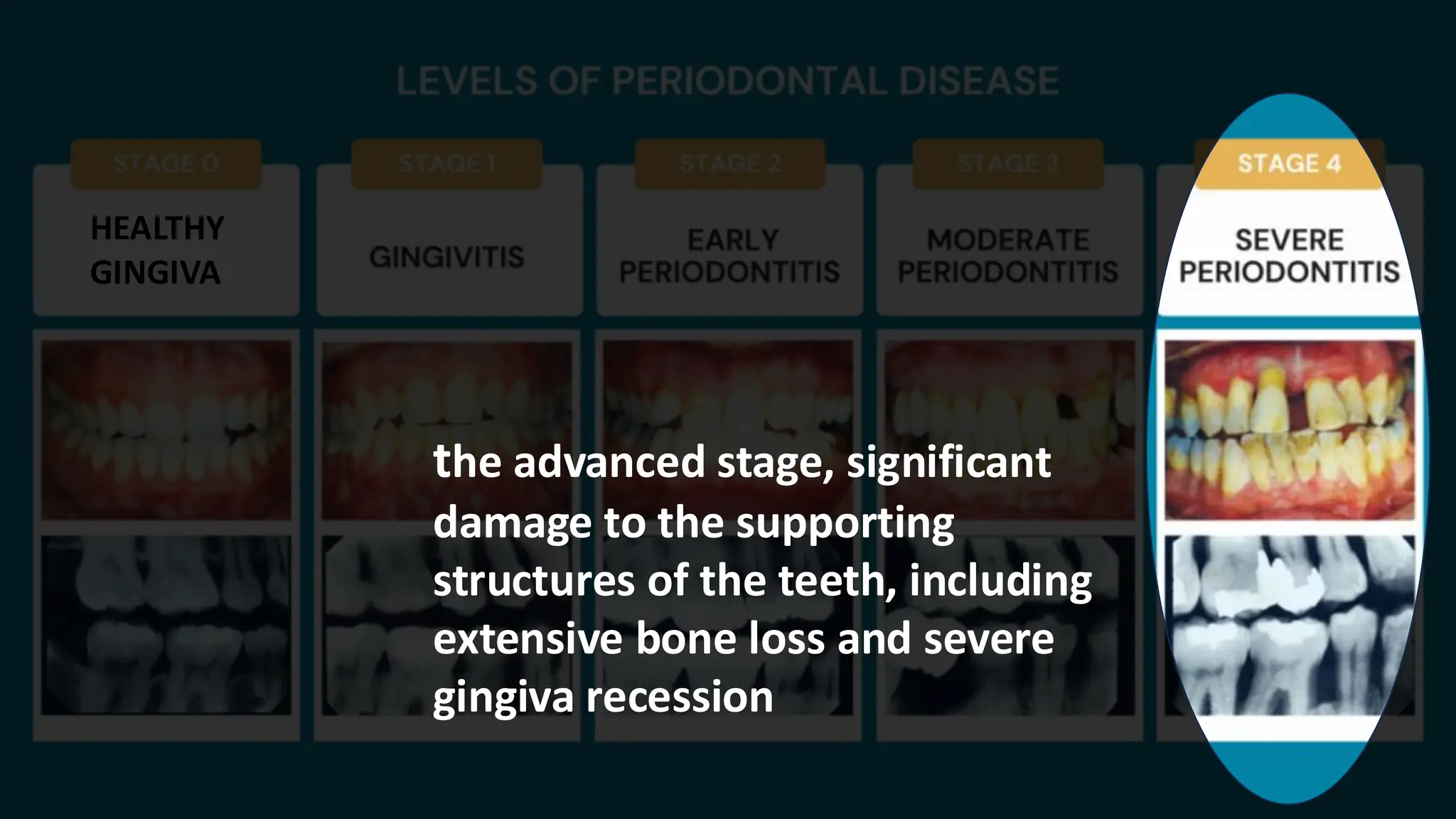
the advanced stage,significant
damage to the supporting
structures of the teeth, including
extensive bone loss and severe
gingiva recession
20.
Can be acuteor chronic:
• Acute: Sudden onset, often
due to a periodontal abscess.
• Chronic: Gradual onset,
commonly associated with
chronic periodontitis.
Acute conditions: Pain is
usually short-lived but intense.
Chronic conditions:Pain can
persist for weeks to months,
often fluctuating in intensity.
Onset
21.
Can be acuteor chronic:
• Acute: Sudden onset, often
due to a periodontal abscess.
• Chronic: Gradual onset,
commonly associated with
chronic periodontitis.
Acute conditions: Pain is
usually short-lived but intense.
Chronic conditions:Pain can
persist for weeks to months,
often fluctuating in intensity.
Duration
22.
Usually described asdull,
throbbing, or aching.
Can be sharp or stabbing in
cases like a periodontal
abscess.
Character
23.
Usually described asdull,
throbbing, or aching.
Can be sharp or stabbing in
cases like a periodontal
abscess.
Mild to moderate in chronic cases.
Severe in acute conditions like
abscesses.
Severity
24.
localized around atooth.
Affects the gingiva, periodontal
ligament, or alveolar bone
surrounding the affected teeth.
Mild to moderate in chronic cases.
Severe in acute conditions like
abscesses.
Location
and Site
25.
localized around atooth.
Affects the gingiva, periodontal
ligament, or alveolar bone
surrounding the affected teeth.
Acute: Sudden onset, severe and
Rapid progression of symptoms.
Chronic: Gradual progression.
Course
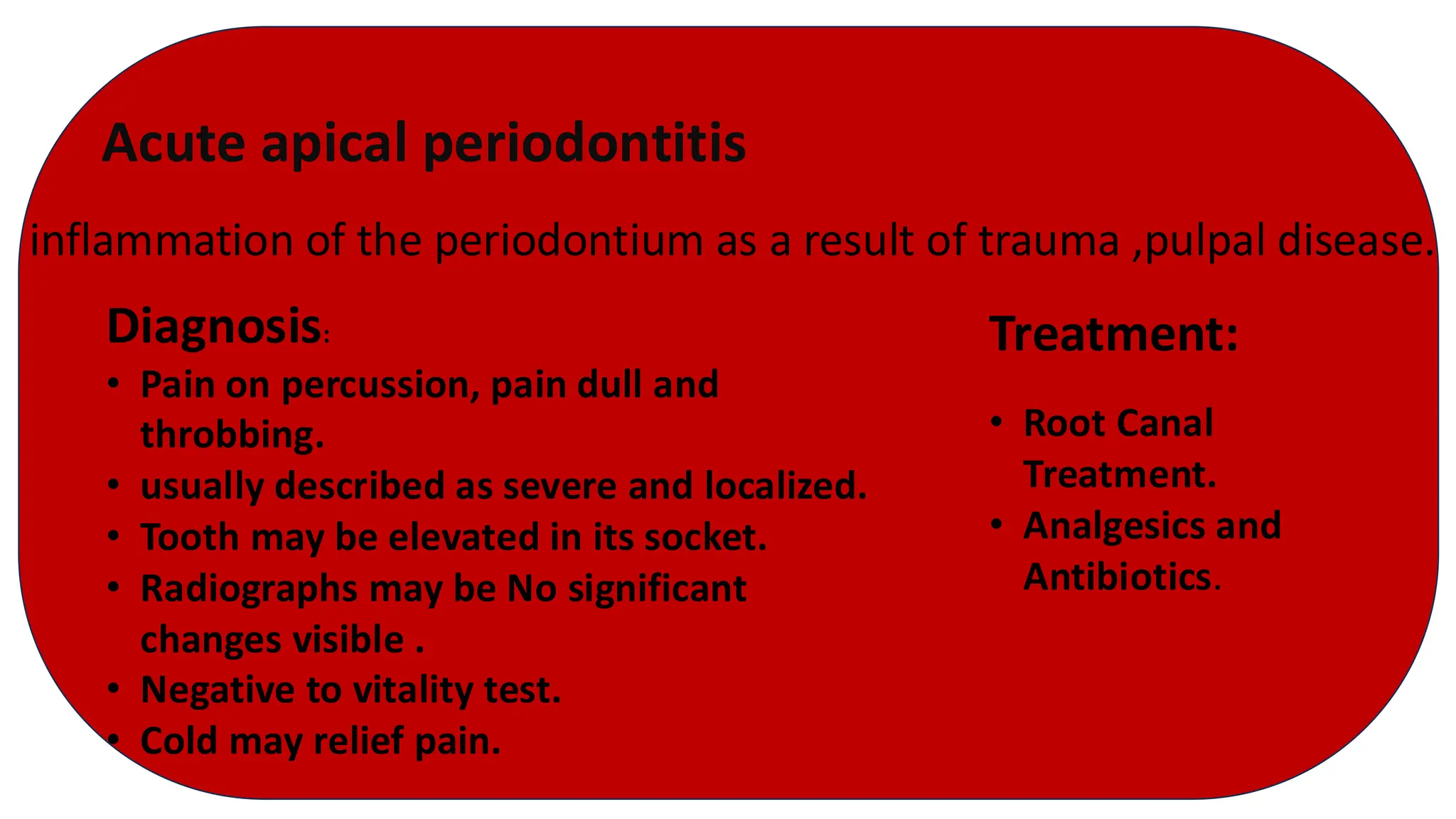
Acute apical periodontitis
inflammationof the periodontium as a result of trauma ,pulpal disease.
Diagnosis:
• Pain on percussion, pain dull and
throbbing.
• usually described as severe and localized.
• Tooth may be elevated in its socket.
• Radiographs may be No significant
changes visible .
• Negative to vitality test.
• Cold may relief pain.
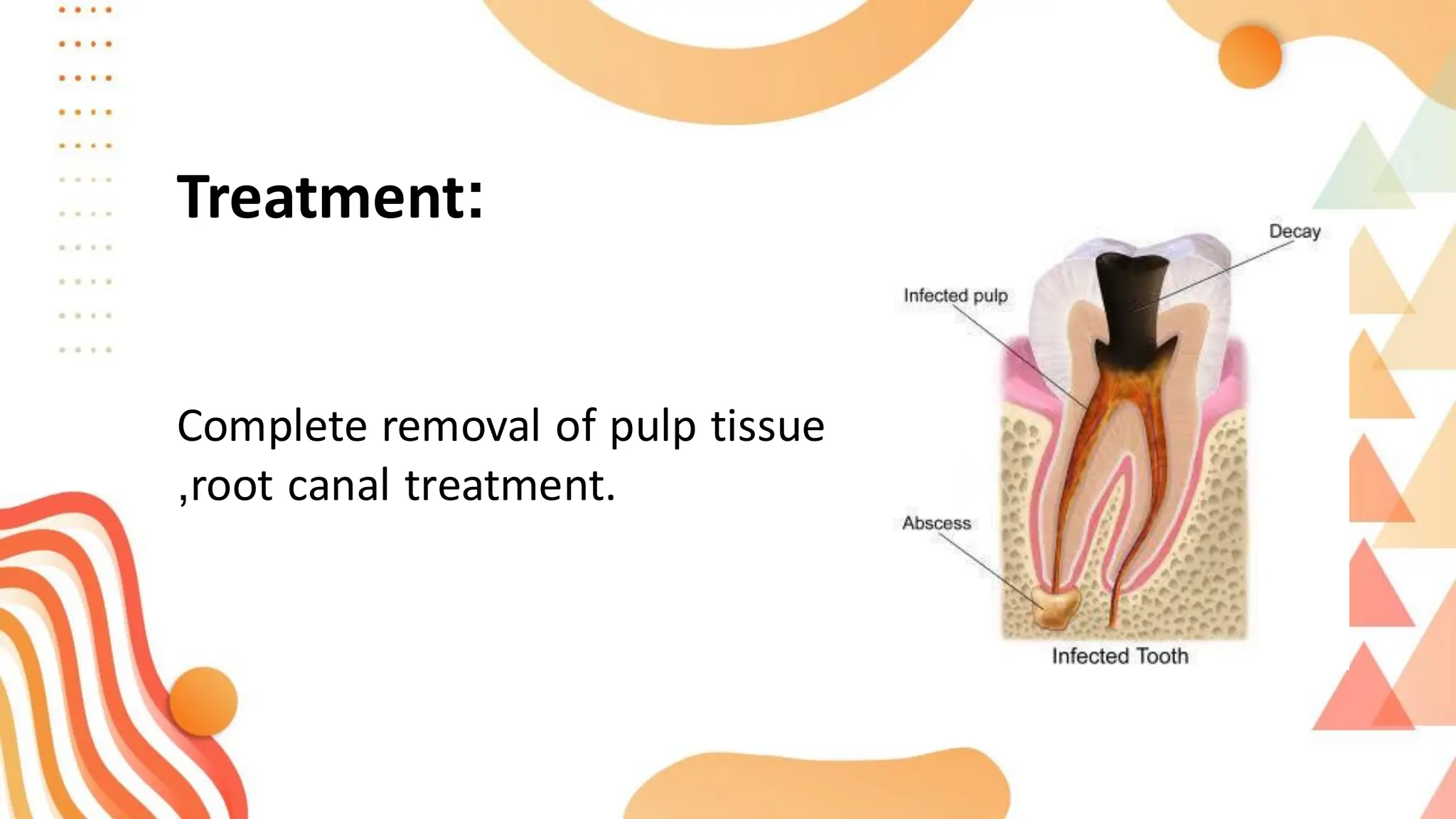
Treatment:
• Root Canal
Treatment.
• Analgesics and
Antibiotics.
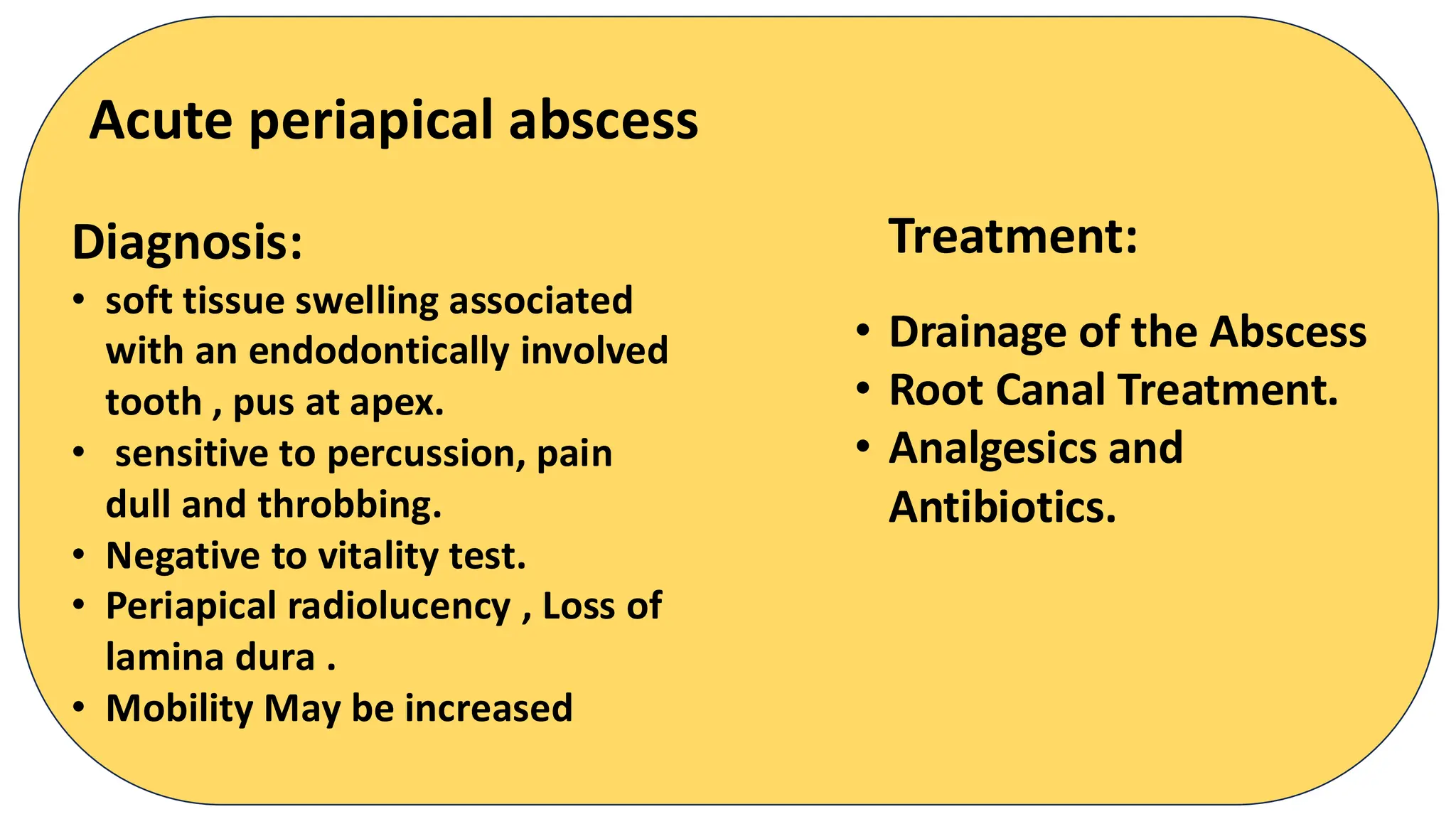
Acute periapical abscess
Diagnosis:
•soft tissue swelling associated
with an endodontically involved
tooth , pus at apex.
• sensitive to percussion, pain
dull and throbbing.
• Negative to vitality test.
• Periapical radiolucency , Loss of
lamina dura .
• Mobility May be increased
Treatment:
• Drainage of the Abscess
• Root Canal Treatment.
• Analgesics and
Antibiotics.
Chronic apical periodontitis:
Diagnosis:
•painless on Percussion.
• Negative to vitality test.
• Periapical radiolucency and
Loss of lamina dura around
the root apex.
• contains granulation tissue.
a long-standing inflammation of the periapical tissues caused by
persistent irritation
Treatment:
• Root Canal Treatment.
• Analgesics and
Antibiotics.
• Follow-Up Care
Chronic Periapical Abscess:
Diagnosis:
•Negative to vitality test.
• Radiolucent area around the
apex of the tooth.
• tenderness on percussion.
• Presence of a draining sinus
tract.
• Necrotic pulp.
Treatment:
• Root Canal Treatment.
• Drainage
• Antibiotics.
• Follow-Up.
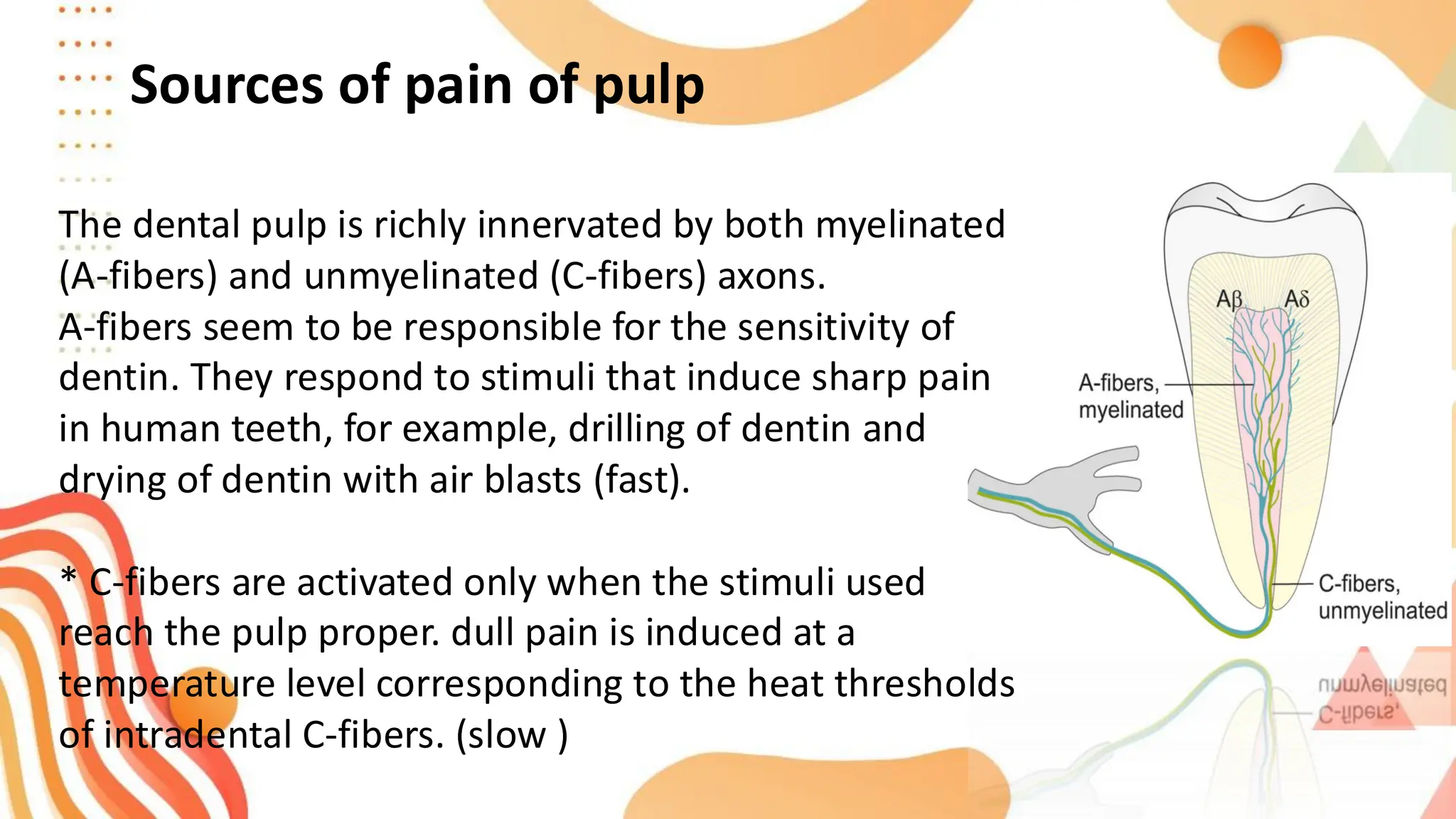
Sources of painof pulp
The dental pulp is richly innervated by both myelinated
(A-fibers) and unmyelinated (C-fibers) axons.
A-fibers seem to be responsible for the sensitivity of
dentin. They respond to stimuli that induce sharp pain
in human teeth, for example, drilling of dentin and
drying of dentin with air blasts (fast).
* C-fibers are activated only when the stimuli used
reach the pulp proper. dull pain is induced at a
temperature level corresponding to the heat thresholds
of intradental C-fibers. (slow )
50.
Pulpitis can beacute occurs when a stimulus (usually cold
or sweet) is applied to the tooth. When the stimulus is
removed, the pain ceases within 1 to 2 seconds.
and can be chronic pulpitis occurs spontaneously or
lingers minutes after the stimulus (usually heat, less
frequently cold) is removed.
the pulp is poorly localised
Caracterized of pulp pain
Dentinal sensitivity
fluid movementswithin exposed dentinal tubules
According to hydrodynamic theory.
Characterized by:
may induce short sharp pain even with only minor
provocation
Gentle touch, mild cold or hot, chemical (acidic or sweet
fruits, foods, drinks) and air-flow stimuli can induce short
sharp pain that may affect daily activities including eating,
drinking, speaking and tooth brushing.
53.
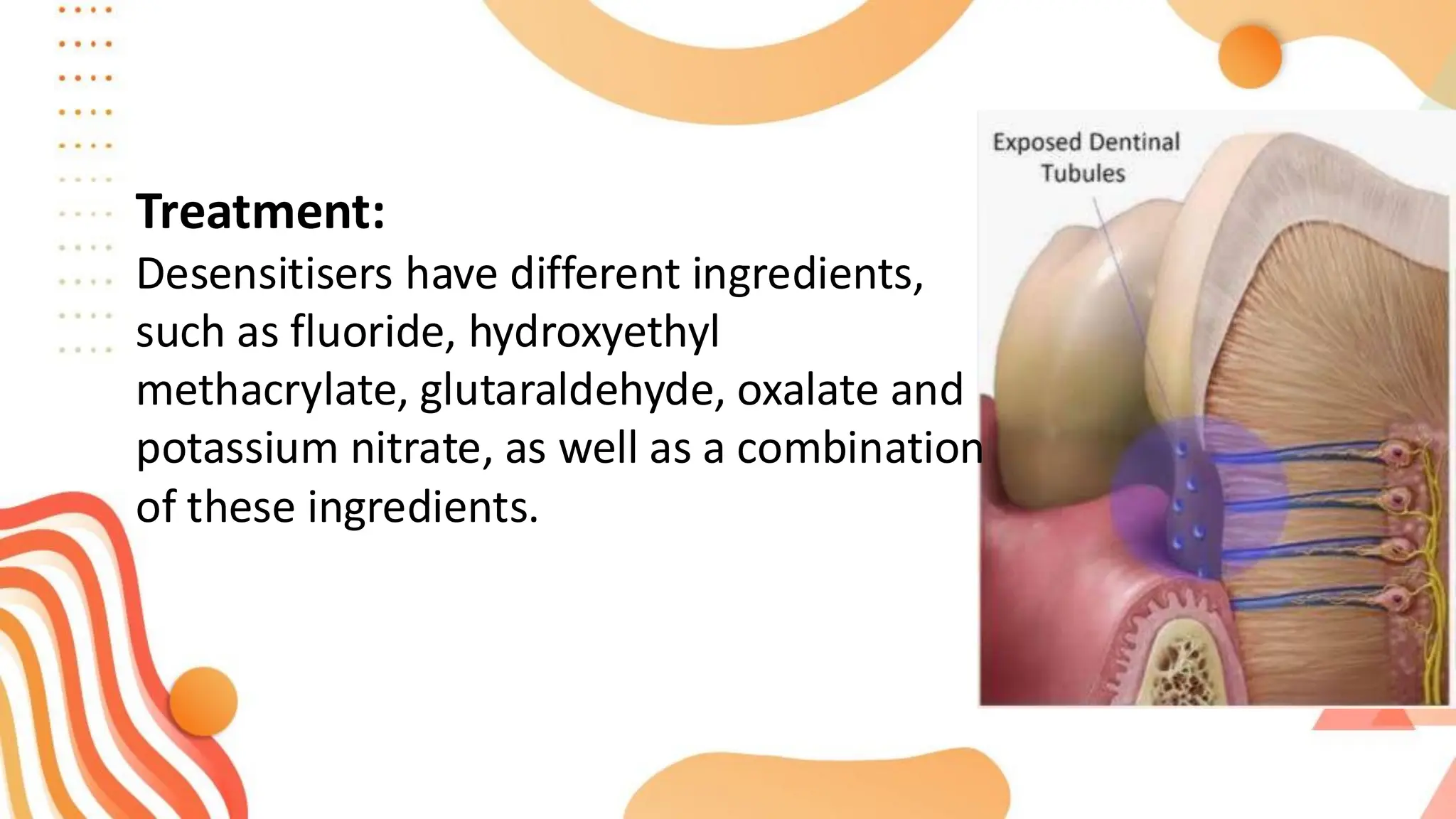
Treatment:
Desensitisers have differentingredients,
such as fluoride, hydroxyethyl
methacrylate, glutaraldehyde, oxalate and
potassium nitrate, as well as a combination
of these ingredients.
54.
Reversible pulpitis
Called pulphyperemia Occur due to deep
caries or by replaced of metallic restoration
without applied base.
55.
Pain type :sharp and momentary pain which
ceases after stimulus is removed
Stimulus: External stimulus, for example, heat,
cold, and sugar
Pain at night : no
Pain localization : Only with applied cold stimulus
or PDL inflammation
Referred pain : usually not found
Diagnosis:
56.
Diagnosis:
Percussion/occlusion
If due toocclusion, percussion test is positive, otherwise
normal.
Vitality test response: exaggerated, brief
a. Tooth respond more severely than healthy teeth and at
lower level of stimulation.
b. Pain lasts for less than 15 second after removal of
stimulus.
c. Tooth responds more to cold than heat stimulation.
57.
Treatment
Remove the irritantor repair tooth structure (caries,
exposed dentin, defective restoration).
Continue to monitor the patient's symptoms.
Advise patient to return if symptoms persist or worsen.
Symptoms of NecroticPulp
Thermal:
No response.
Sweets:
No response.
:
Biting Pressure
Usually moderate to severe pain not symptom of necrotic
pulp, but rather periapical inflammation.
Moderate to severe spontaneous pain usually dull and
throbbing; associated with periapical area
61.
Diagnosis of NecroticPulp
Distinguishing features:
-No response to cold.
-No response to pulpal test.
Caveats
-Decreased sensitivity to cold/ept may be from of insulating effects
of additional dentin.
-Fluid in canal space conducting electrical current can give false-
positive.
62.
Pulp necrosis
Death ofthe pulp may result from an untreated irreversible pulpitis or
from traumatic injury that disrupts the blood supply to the pulp.
It can be partial N. which gives similar symptoms to irreversable pulpitis
or total N. which is asymptomatic.
If not treated it will spread beyond the apical foramen causing
inflammation of the periodontal ligament; result in thickening of
periodontal ligament, which may be quit sensitive to percussion















![Presentation1 [Autosaved].pdf diagnosiss](https://image.slidesharecdn.com/presentation1autosaved-250812162634-6365894a/75/Presentation1-Autosaved-pdf-diagnosiss-64-2048.jpg)















































