Downloaded 27 times
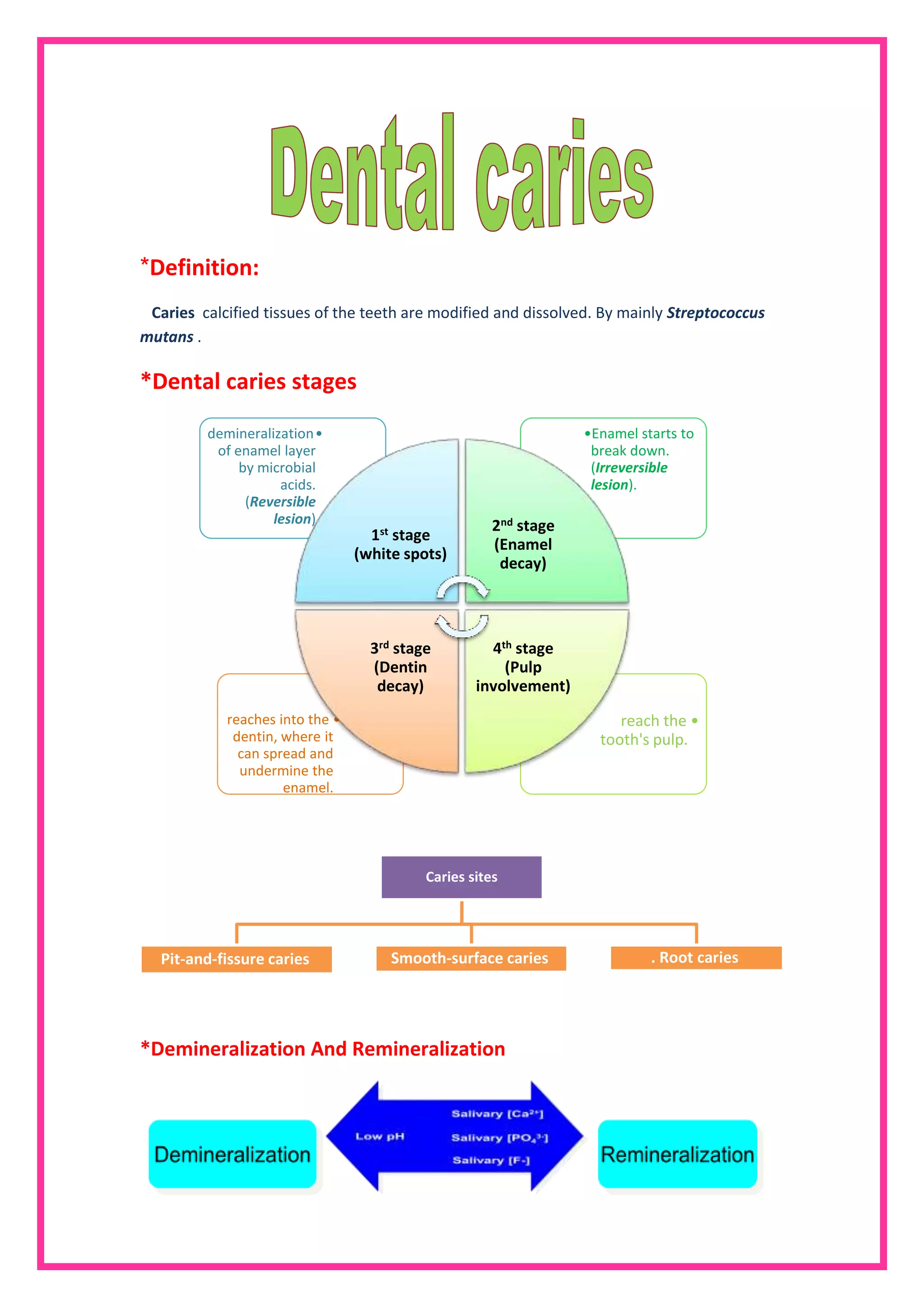


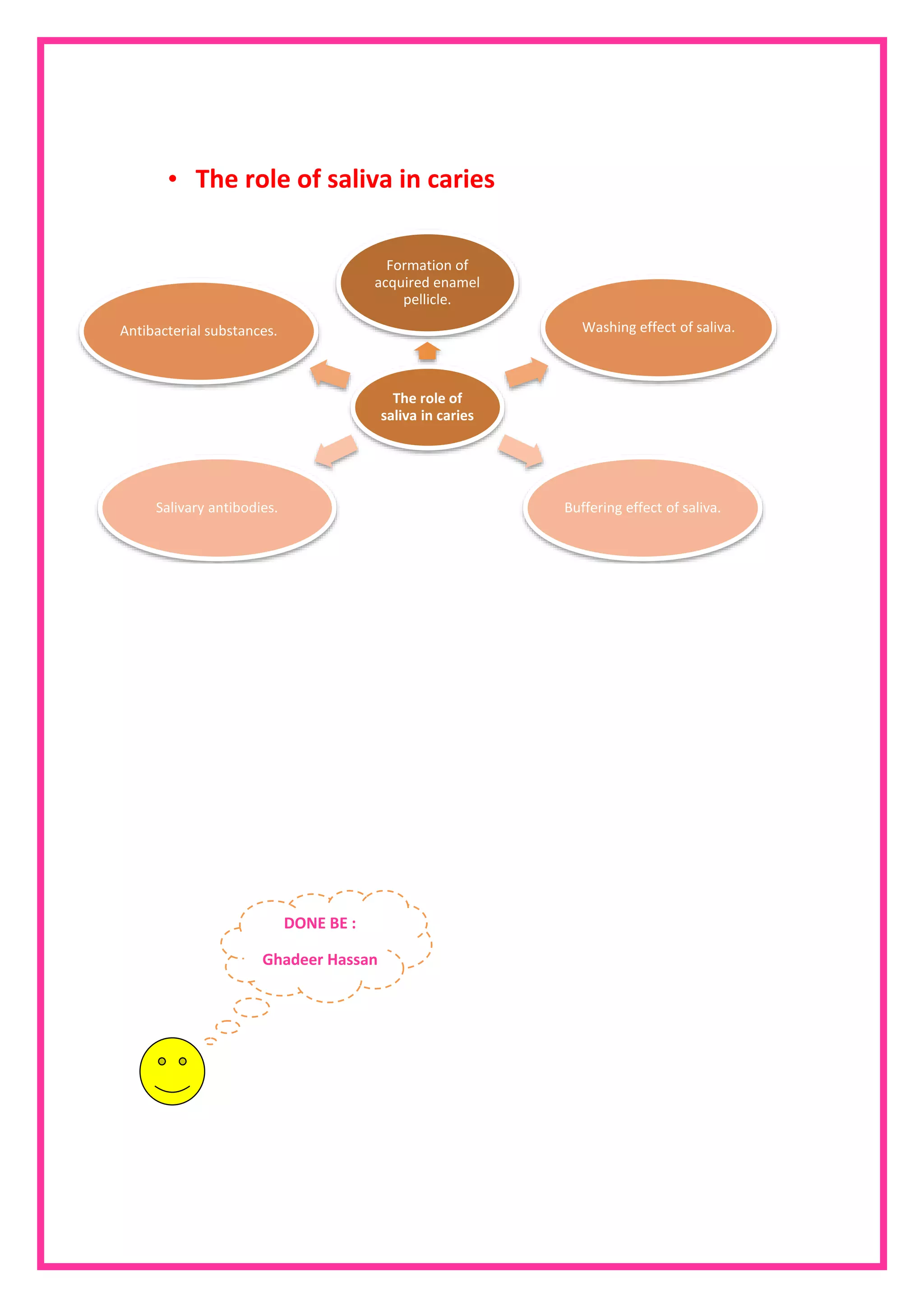

The document discusses dental caries, emphasizing the role of Streptococcus mutans in the demineralization process of tooth tissues. It outlines the stages of caries progression from white spots to pulp involvement, as well as the factors influencing caries development, including microbial presence and dietary sugars. Additionally, it highlights the importance of saliva in dental health, serving protective functions against caries.









![Anatomical landmarks of maxilla and mandible [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/anatomicallandmarksofmaxillaandmandibleautosaved-200820132830-thumbnail.jpg?width=640&height=640&fit=bounds)
























































































