Downloaded 37 times


![Essential requirements for development of dental caries :
1.
Cariogenic (acidogenic)
bacteria
[ These are viridans streptococci which are a heterogeneous
group including Streptococcus mutans, S. sobrinus, S. salivarius,
S. mitior and S. sanguis
and lactobacilli. ]](https://image.slidesharecdn.com/dc-170524192254/85/Dental-Caries-A-Presentation-by-MunabbiR-8-320.jpg)
![Essential requirements for development of dental caries :
2.
Bacterial plaque
[Dental plaque is a biofilm or mass of bacteria that grows on
stagnation areas of tooth surface , usually sticky & colorless
and gradually becoming harder & brownish resulting in tooth
decay. ]](https://image.slidesharecdn.com/dc-170524192254/85/Dental-Caries-A-Presentation-by-MunabbiR-9-320.jpg)
![Essential requirements for development of dental caries :
3.
Stagnation areas
[The location on the surface of a tooth where there is
a tendency for food debris to accumulate. ]](https://image.slidesharecdn.com/dc-170524192254/85/Dental-Caries-A-Presentation-by-MunabbiR-10-320.jpg)
![Essential requirements for development of dental caries :
5.
Susceptible tooth surfaces
[ Some tooth surfaces are more susceptible or vulnerable to
form and develop plaque and caries, depending on enamel
structure & mineral+fluoride contents ]](https://image.slidesharecdn.com/dc-170524192254/85/Dental-Caries-A-Presentation-by-MunabbiR-12-320.jpg)
![Essential requirements for development of dental caries :
6.
Time
[ If time is provided to the causing bacteria by not treating
them, they spontaneously multiply and form plaque followed
by caries ]](https://image.slidesharecdn.com/dc-170524192254/85/Dental-Caries-A-Presentation-by-MunabbiR-13-320.jpg)
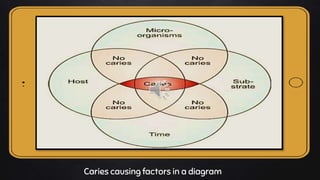
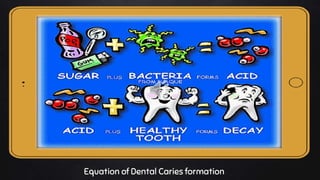











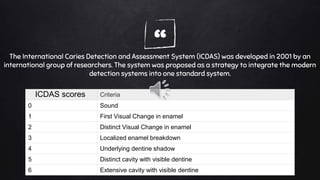





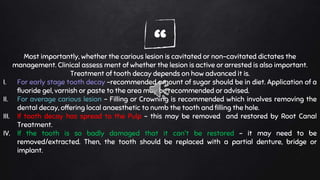





Dental caries, or tooth decay, is a microbial disease caused by bacteria in the mouth that leads to demineralization of tooth enamel and dentin. Key factors for development of caries include cariogenic bacteria, bacterial plaque, fermentable carbohydrates, and susceptible tooth surfaces. Symptoms may include tooth sensitivity, pain, and visible cavities. Diagnosis involves visual examination and sometimes x-rays. Treatment depends on the severity but may include fillings, root canals, extractions, or replacements like bridges or implants. Maintaining good oral hygiene through regular brushing and cleanings can help prevent caries.




































![DENTAL CARIES[1].pptx related to dental decay](https://cdn.slidesharecdn.com/ss_thumbnails/dentalcaries1-250825004011-3d4a03c6-thumbnail.jpg?width=640&height=640&fit=bounds)






























