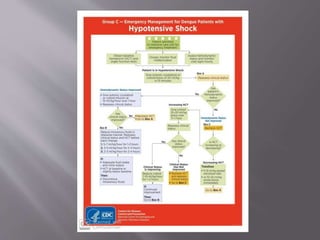
This document discusses dengue fever, caused by dengue virus transmitted by mosquitoes. It covers the epidemiology, pathophysiology, clinical presentation, diagnosis, treatment and prevention of dengue fever. Dengue virus infects 50 million people annually worldwide, with Southeast Asia having millions of infections and thousands of deaths each year. Dengue fever symptoms include fever, headache, joint pains and rash. More severe dengue hemorrhagic fever and dengue shock syndrome can occur and require hospitalization and fluid replacement therapy. Prevention focuses on controlling mosquito vectors and avoiding mosquito bites.



























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








