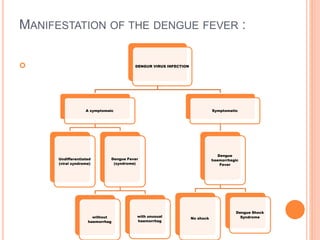
Dengue fever is caused by any of four related dengue virus serotypes transmitted by Aedes mosquitoes. It manifests as a sudden onset of fever, headache, muscle and joint pains. In some cases it can progress to severe dengue hemorrhagic fever or dengue shock syndrome, characterized by bleeding, low blood pressure and organ failure. There is no vaccine or specific antiviral treatment, so management focuses on relief of symptoms and careful fluid replacement to prevent shock. Prevention relies on controlling mosquito populations and avoiding mosquito bites.


![INTRODUTION:
Dengue Virus – One of four closely related but
antigenic ally distinct virus serotypes.
[DEN-1,DEN-2,DEN-3 & DEN-4] of the genus Flavi
Virus.
Dengue Fever is transmitted by the bite of an
Aedes mosquito infected with a Dengue Virus.
when it bites a person with engue virus in their
blood.](https://image.slidesharecdn.com/deguefever13-210305065232/85/Degue-fever-3-320.jpg)
![HISTORY:
In 15th to 19th Centuries – A aegypti spread out of Africa.
In 1779 & 1780 – Spread to Aisa, Africa & North
America.
Until 1940 – In frequent epidemics outbreaks.
1906- confirmed that transmission by the Aedes
mosquitoes.
During and after 2nd World War – attributed to ecologge
disruption
1953 – sever form of diseases first reported in
Philippines.
1970- It become a major cause of child mortality.
Till 2014-there is a long intervals [10-40 years] between
major epidemics.](https://image.slidesharecdn.com/deguefever13-210305065232/85/Degue-fever-6-320.jpg)
![ Dengue is an actue viral infection caused by atleast
4 serotypes [1,2,3 & 4] of dengue virus
It occur epidemically or endemically.
It start during the rainy season when the breeding
of the vector mosquitoes in generally abundant.
Temperature also plays an important role in the
transmission of dengue virus by mosquitoes.
Mosquitoes kept at 260 Celsius fail to transmit
DEN-2 Virus.](https://image.slidesharecdn.com/deguefever13-210305065232/85/Degue-fever-10-320.jpg)