Downloaded 115 times

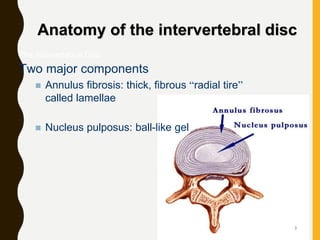
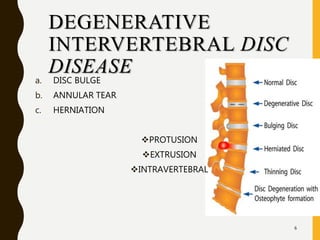













1. The document discusses degenerative disc disease, which describes the natural breakdown of an intervertebral disc in the spine. As discs degenerate, they lose water and proteoglycan content, collagen fibers become distorted, and tears can occur, resulting in decreased disc height, impaired mobility, and pain. 2. Degenerative disc changes include disc bulges, annular tears (concentric, radial, transverse), and herniations (protruded, extruded, intravertebral). Herniations involve the displacement of disc material beyond the disc space. 3. MRI is the best method for diagnosing degenerative disc conditions. Management includes therapeutic exercises and medical treatment.























































































