Downloaded 222 times






























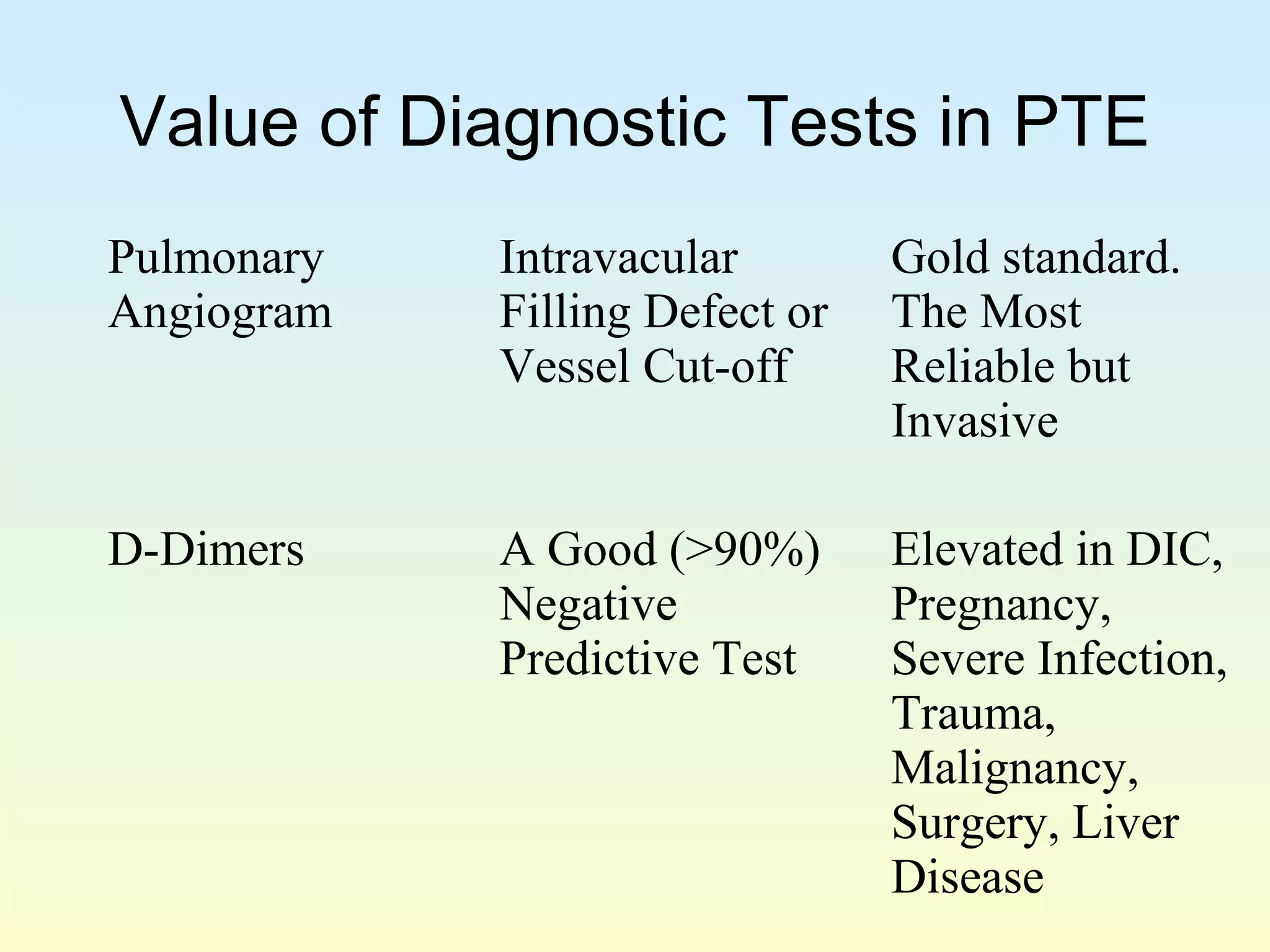




























































The document provides information on deep vein thrombosis and pulmonary embolism. It discusses: 1. The coagulation process and how abnormalities in the vessel wall, blood flow, or blood components can lead to thrombosis according to Virchow's triad. 2. Risk factors for deep vein thrombosis and pulmonary embolism such as age, cancer, immobilization, and inherited conditions. 3. Diagnostic tests for pulmonary embolism including the Wells criteria for estimating probability, imaging tests like CT scans, and their limitations. Treatment involves anticoagulants like heparin or warfarin.























































































