This document discusses fetal anomalies that can be detected in the first trimester via ultrasound screening. It provides examples of several major anomalies like anencephaly, acrania, holoprosencephaly, cephalocele, micrognathia, diaphragmatic hernia, bladder exstrophy, and body stalk anomaly that can be diagnosed in the first trimester. While some structures like the spine and limbs may be difficult to evaluate, ultrasound has improved to allow detection of a wide range of abnormalities from 11-14 weeks gestation. Follow up scans in the early second trimester can provide further diagnosis when initial findings are suspicious but not definitive.
Introduction to fetal anomalies in the first trimester, ultrasound diagnostics, and screening methods including NT measurements for chromosomal abnormalities.
Focus on anencephaly, its incidence, sonographic features and early detection using ultrasound.
Describes acrania, its rarity, incidence, and ultrasound diagnostics indicating absence of skull structure.
Discussion on holoprosencephaly, prevalence, types, and how ultrasound identifies this malformation.
Details cephalocele, its incidence, and ultrasound findings for CNS herniation through skull defects.
Micrognathia condition, its prevalence, ultrasound diagnostics including features of the lower jaw.
Diaphragmatic hernia prevalence and ultrasound diagnosis showing abdominal contents herniated into thorax.
Focus on body stalk anomaly, its prevalence, and diagnostic ultrasound findings related to severe defects.
Common abdominal structures and defects in the first trimester, distinguishing physiologic from pathological anomalies.
Evaluation of spine and limb structures in the first trimester, discussing potential anomalies like spina bifida.
Importance of early ultrasound for prenatal diagnosis to ensure timely abortion decisions before routine second-trimester scans.
• From the1st day of last menstrual cycle to 12th week of pregnancy.
• Ultrasound is the main screening and diagnostic tool for congenital
structural abnormalities.
• With improvement in the resolution of ultrasound machines and wide
application of the nuchal translucency (NT) scan, it is possible to delineate
normal fetal anatomy and diagnose a wide range of fetal abnormalities in
the first trimester. (1) Measurement of NT thickness between 11 and 14
weeks gestation, combined with maternal age and maternal serum
biochemistry, can be an effective method of screening for trisomy 21 and
other chromosomal abnormalities. Besides nuchal abnormalities, a wide
range of other congenital anomalies can be diagnosed with ultrasound at
11-14 weeks gestation, including defects of the central nervous system,
heart, anterior abdominal wall, urinary tract, and skeleton.
3.
• In thefirst trimester, some major anomalies can be diagnosed or
excluded. In other cases, there may be findings that are not
diagnostic but that may suggest a structural anomaly. In these
patients, second-trimester ultrasound before 18 weeks can lead to
earlier prenatal diagnosis. Abnormal NT in a fetus with a normal
karyotype is associated with a higher rate of structural abnormalities.
When NT is abnormal, it is reasonable to assess fetal anatomy early in
the second trimester, as some structural anomalies can be identified
prior to 18 weeks’ gestation
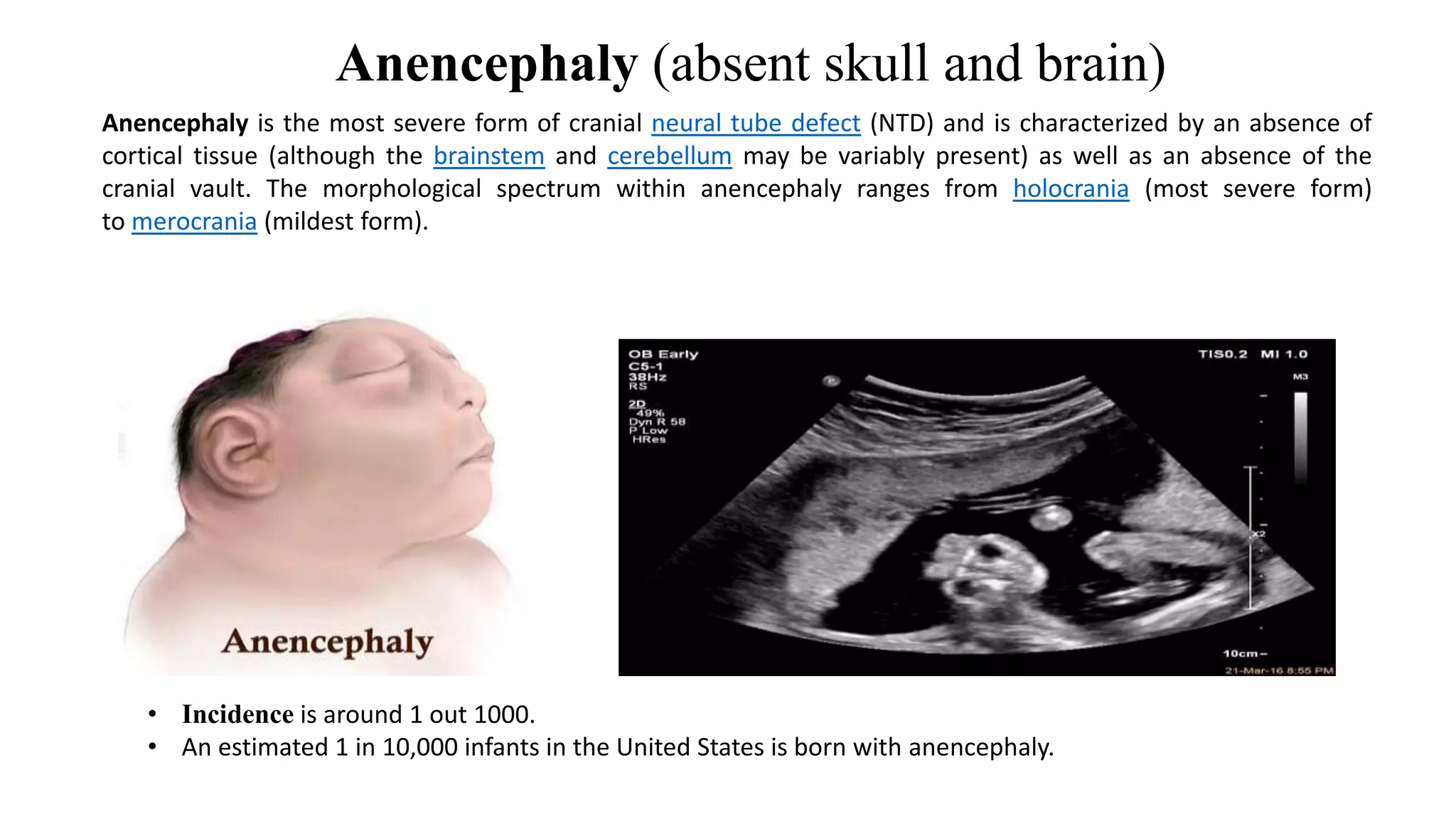
Anencephaly (absent skulland brain)
• Incidence is around 1 out 1000.
• An estimated 1 in 10,000 infants in the United States is born with anencephaly.
Anencephaly is the most severe form of cranial neural tube defect (NTD) and is characterized by an absence of
cortical tissue (although the brainstem and cerebellum may be variably present) as well as an absence of the
cranial vault. The morphological spectrum within anencephaly ranges from holocrania (most severe form)
to merocrania (mildest form).
6.
Sonographic Features
• Anencephalymay be sonographically detectable as early as 11
weeks. Ultrasound can be a non-invasive, cost effective and fast method to
detect anencephaly and has an accuracy of approximately 100% at 14
weeks. Sonographic features of anencephaly include:
• no parenchymal tissue is seen above the orbits and calvarium is absent:
parts of the occipital bone and mid brain may be present
• if a small amount of neural tissue is present, it is then termed exencephaly
• this may be seen at an earlier stage
• less than expected value for crown rump length (CRL)
• a "frog eye" or "mickey mouse" appearance may be seen when seen in the
coronal plane due to absent cranial bone/brain and bulging orbits.
• may show evidence of polyhydramnios: due to impaired swallowing
7.
Acrania (absent skull)
Acraniais a rare congenital disorder that occurs in the human fetus in which the flat bones in the cranial vault are
either completely or partially absent.
Incidence
Although acrania associated with anencephaly is a well recognized entity with an incidence of about 10:10,000 births.
Six of our seven fetuses in which the sex was reported were females and one male.
8.
Ultrasound diagnosis:
• Absenceof cranial vault and cerebral hemispheres.
• At 12 weeks acrania is suspected by absence of the normally ossified
skull and distortion of the brain (exencephaly). At >16 weeks the brain
is destroyed (anencephaly).
9.
Holoprosencephaly
• Holoprosencephaly (HPE)is a rare congenital brain malformation resulting
from incomplete separation of the two hemispheres.
• Late in the first trimester, the brain can be imaged in the transverse plane,
identifying both hemispheres and midline structures.,, and (no division into
separate hemispheres, with absence of midline structures, If a transverse
view through the fetal brain identifies a normal midline, representing the
falx cerebri, and lateral ventricles, these 3 conditions can be excluded.
10.
• Prevalence:
• 1in 1,300 fetuses at 12 weeks’ gestation.
• 1 in 10,000 births.
• Ultrasound diagnosis:
• Abnormalities from incomplete cleavage of the forebrain observed in
the standard transverse sections of the brain.
• There are 3 types:
• Alobar: fusion of the cerebral hemispheres with a single ventricle.
• Semilobar: cerebral hemispheres and lateral ventricles are fused anteriorly
but separated posteriorly.
• Lobar: cerebral hemispheres are separated both anteriorly and posteriorly,
but there is partial fusion of the frontal horns of the lateral ventricles,
absence of septum pellucidum and abnormalities of the corpus callosum,
cavum septum pellucidum and olfactory tract.
11.
Cephalocele : Alarge skull defect
• Cephalocele refers to the outward herniation of CNS contents
through a defect in the cranium. The vast majority are midline.
• The estimated incidence is 0.8-4:10,000 live births
• Ultrasound diagnosis:
•Subjective finding of prominent upper lip and receding chin in the
mid-sagittal view of the face. These findings may be due to
micrognathia (short mandible) or retrognathia (backward
displacement of the mandible).
• Severe micrognathia is associated with polyhydramnios (>25 weeks’
gestation), due to glossoptosis (normal tongue obstructing small oral
cavity).
16.
Diaphragmatic hernia
• Prevalence:
•1 in 4,000 births.
• Ultrasound diagnosis:
• Abdominal viscera herniated into the thorax through defect in the
diaphragm with associated deviation of the heart from its normal
position.
• Bowel, stomach and / or liver in the thorax.
17.
• Bladder exstrophy
•Prevalence:
• 1 in 30,000 births.
• More common in males than in females: 2 to 1.
• Ultrasound diagnosis:
• Abdominal wall mass in the suprapubic region below a low insertion
of the umbilical cord.
• Non-visible bladder with normal volume of amniotic fluid.
• Widely separated pubic bones, short and broad penis in males,
hemiclitoris on either side of the bladder in females.
18.
• Body stalkanomaly
• Prevalence:
• 1 in 10,000 pregnancies.
• More often in a younger age group and cocaine abuser.
• Ultrasound diagnosis:
• Presence of a major abdominal wall defect, severe kyphoscoliosis and
short or absent umbilical cord. Typically, the liver is directly attached
to the placenta without interposed umbilical cord and there is major
distortion of the spine.
19.
Abdomen
• In thefirst trimester, visible structures include the ventral wall,
umbilical cord insertion, stomach bubble, and urinary bladder. The
most common abnormalities identified are the ventral wall defects
omphalocele, gastroschisis, and more extensive defects including
body-stalk anomaly and limb-body-wall complex. Physiologic midgut
herniation is common prior to 12 weeks’ gestation and should not be
confused with an omphalocele. An enlarged urinary bladder
(megacystis) can represent early evidence of bladder outlet
obstruction. Kidneys are generally not imaged at < 14 weeks, and
because amniotic fluid does not consist primarily of fetal urine until
the second trimester, absent or dysfunctional kidneys will not result
in oligohydramnios earlier in pregnancy.
20.
Spine
• The spineis not easy to evaluate in the first trimester, and most
abnormalities will go undetected. Spina bifida involving multiple
levels can be suspected in rare cases, as can large masses such as
sacrococcygeal teratoma.
21.
Limbs
• At aminimum, all limbs should be documented, including proximal
long bones (humerus and femur) and distal long bones (radius/ulna
and tibia/fibula). Severe skeletal dysplasias, such as thanatophoric
dysplasia, can have features such as small limbs and narrow chest
even in the first trimester. Hands and feet can also be imaged,
although abnormalities of the digits cannot always be identified. In
some cases, polydactyly may be suspected.
22.
• In somecases, first-trimester ultrasound findings may be suspicious,
but not diagnostic, for abnormalities of certain structures. In these
cases, early second-trimester ultrasound can lead to prenatal
diagnosis prior to the routine 18- to 20-week scan. In our experience,
early second-trimester ultrasound in such cases contributed to lower
gestational age at abortion in women undergoing ultrasound at 11 to
14 weeks.