Downloaded 170 times


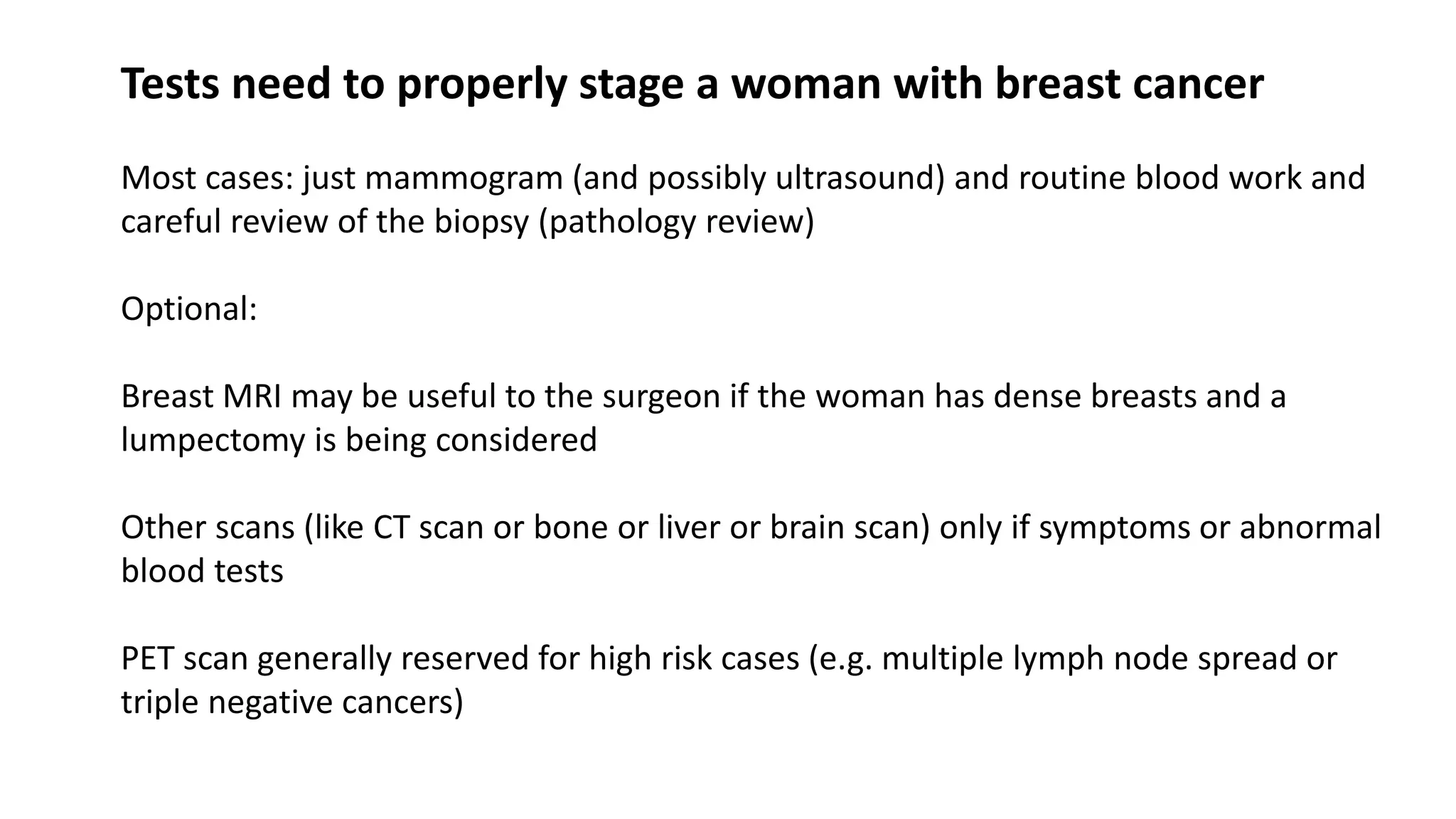

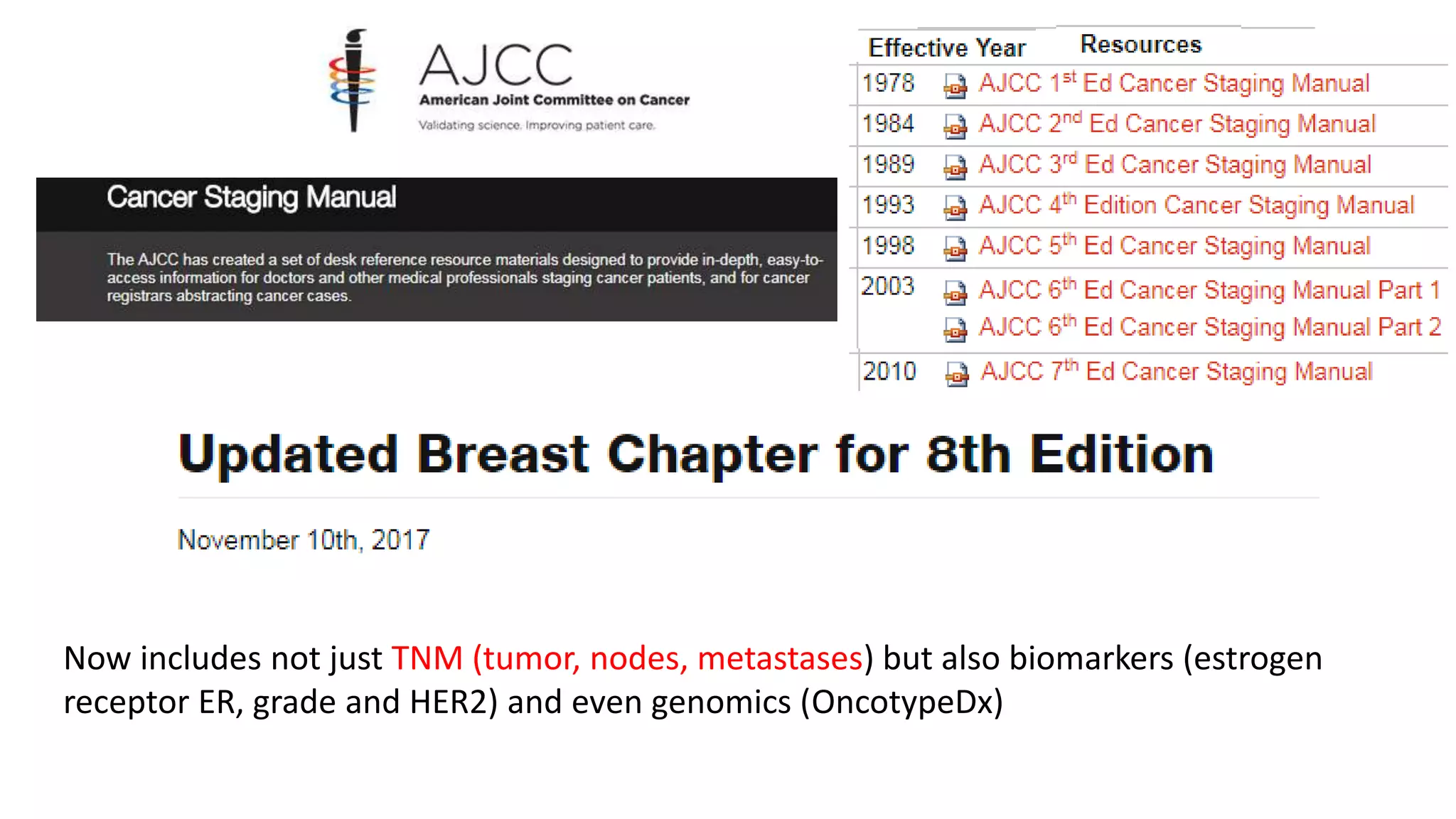














































Tests needed to stage breast cancer typically include a mammogram, ultrasound, and bloodwork. Additional tests like an MRI, CT, bone scan, or PET scan may be used depending on symptoms or abnormal results. Staging also considers tumor size and spread (TNM system), along with biomarkers like hormone receptors. Genomic testing can provide information on cancer characteristics and risk of recurrence. Treatment is tailored based on all available information, with clinical and genomic factors both considered. Higher risk cases based on multiple factors may benefit most from chemotherapy in addition to hormone therapy.























![HEREDITARY BREAST and OVARY CANCER [HBOC] SYNDROME, Dr BUI DAC CHI.](https://cdn.slidesharecdn.com/ss_thumbnails/hboc1-150312034459-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)































































