Downloaded 54 times












































































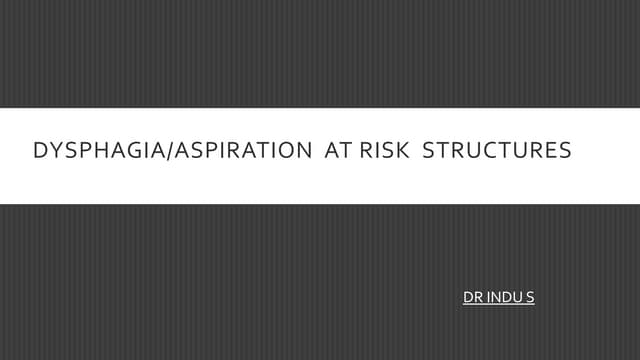
![Intraoperative Technique
Distance
Surface
PE probe (Gy) Conventional EBRT
Physical
Dose
BED Physical
Dose
BED
0.1 cm 15 165 50 60
0.5 cm 8.75 59 50 60
1.0 cm 5.0 21.7 50 60
BED= Physical Dose x [1+ (dose/fx) / a/b)]
a/b = 10 (early effects conventional EBRT)
a/b= 1.5 (assumed for TARGiT device)
Physical Dose Profile
Vaidya et al, Annals of Oncol, 2001; 12: 1075-1080](https://image.slidesharecdn.com/intraoperativeradiotherapycarcinomabreast-180521175602/75/Intraoperative-radiotherapy-carcinoma-breast-78-2048.jpg)















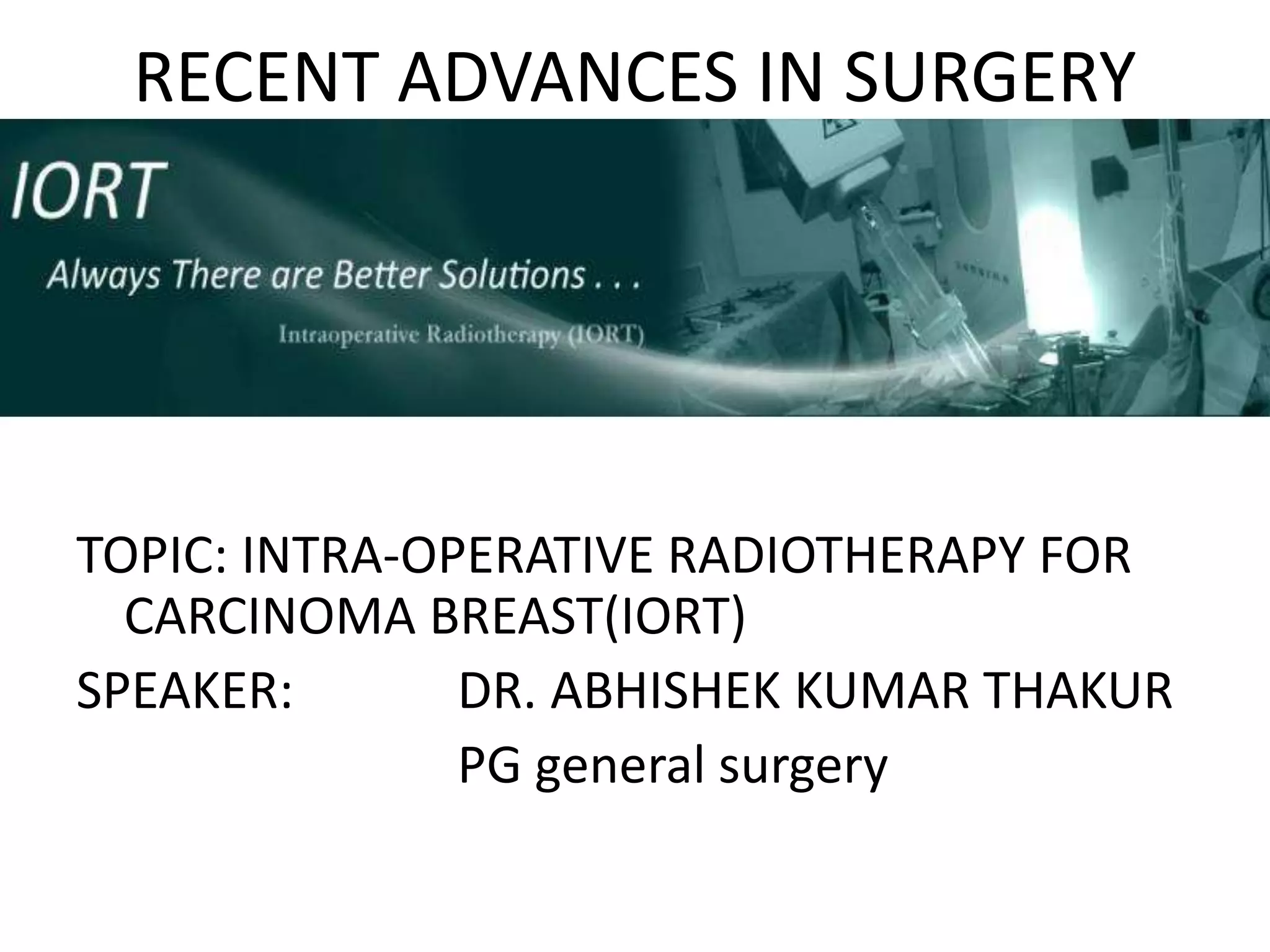
![[S4-2] Targeted Intraoperative Radiotherapy for
Early Breast Cancer: TARGIT-A Trial- Updated
Analysis of Local Recurrence and First Analysis of
Survival
Lancet 2010](https://image.slidesharecdn.com/intraoperativeradiotherapycarcinomabreast-180521175602/75/Intraoperative-radiotherapy-carcinoma-breast-94-2048.jpg)
































This document discusses intra-operative radiotherapy (IORT) for breast cancer. It provides background on breast cancer risk factors, diagnosis, staging, and treatment options. It then describes IORT specifically, noting that it allows targeted radiation to be delivered during surgery directly to the tumor bed in one session using a miniature X-ray source. The technique aims to complete local radiation treatment immediately while avoiding six weeks of daily external beam radiotherapy. Details are provided on the Intrabeam system and applicators used to deliver a uniform radiation dose in a spherical field confined to the tumor bed.