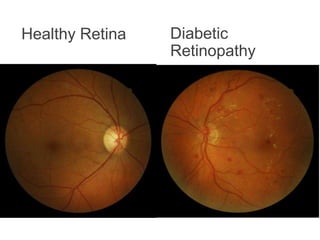
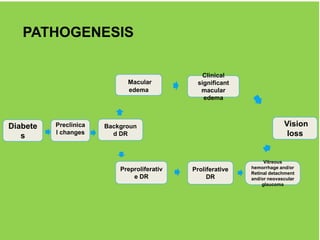
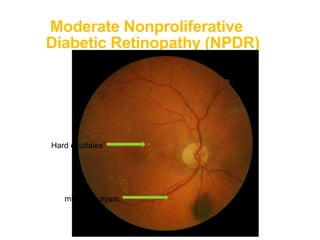
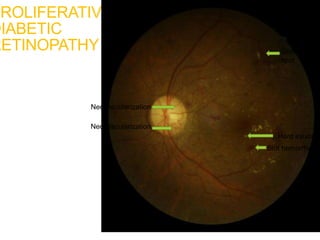
Diabetic retinopathy is a complication of diabetes that affects the small blood vessels in the retina. It is the leading cause of blindness in working age adults. Strict control of blood sugar and blood pressure can help prevent and slow the progression of diabetic retinopathy. Annual eye exams are important for early detection and treatment if needed to prevent vision loss. As diabetic retinopathy progresses, it is classified into mild, moderate, and severe non-proliferative stages and proliferative stage. Treatments include laser therapy and anti-VEGF injections to prevent further vision loss.