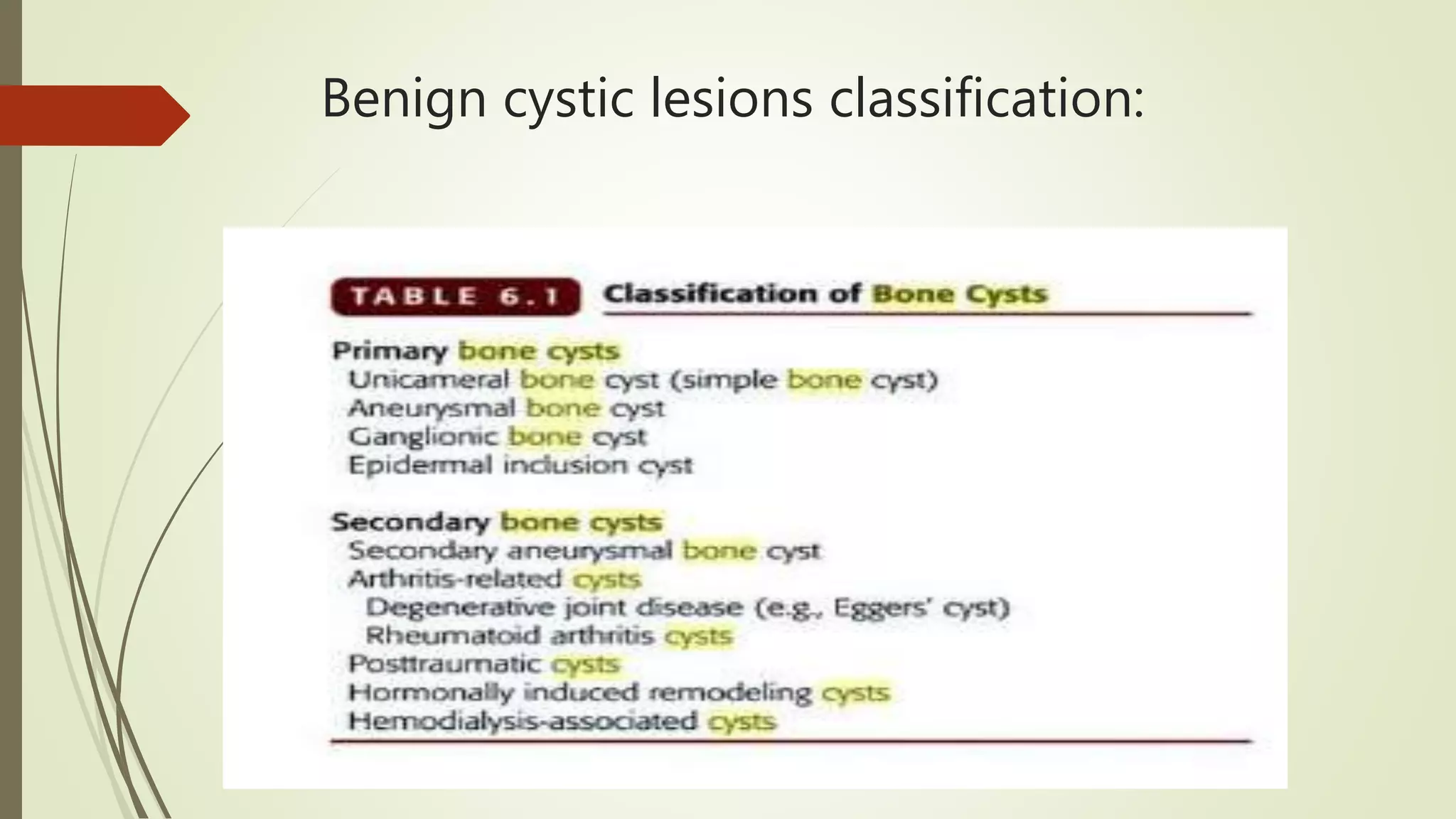
This document provides an overview of the approach to cystic bone lesions. It begins with definitions and classifications of benign and malignant cystic bone lesions. Key aspects to consider in the approach include the age of the patient, location of the lesion, characteristics of the transitional zone, presence of a matrix, status of the bone cortex, periosteal reaction, and soft tissue swelling. Specific cystic lesions discussed individually include aneurysmal bone cyst, solitary bone cyst, fibrous dysplasia, and enchondroma. Treatment approaches are also summarized for some of the lesions.