OVERVIEW OF CTIMAGING AND ITS
IMPORTANCE IN BRAIN DIAGNOSTICS.
CT Brain provides cross-sectional views of the brain’s structure
It helps in identifying traumatic damage, bleeding and infections affecting
the brain with great accuracy
CT Angiography helps in evaluating blood vessels, detecting aneurysms,
blockages and malformations of the brain
It provides support in early diagnosis and improves treatment outcome
significantly.
3.
PATIENT PREPARATION, POSITIONING
ANDEQUIPMENTS
Ensure fasting of the patient and remove all metal objects
Patient is supine with head straight and secured in headrest
Align laser light with anatomical landmarks for precise positioning
Perform a scout image to verify the positioning
CT scanner is set according to protocol and imaging requirements
4.
CT SETTINGS
ImageMode : Use axial or helical mode
Slice Thickness : Set between 0.6 - 5 mm
Scan Range : Covers the region under interest
Tube Voltage : Commonly set at 150 kVp
Tube Current : Adjust based on patient size, between 200 to 400 mA
Scan Timing : Dependent on organ under review
Reconstruction Algorithm
Post processing
5.
RECONSTRUCTION ALGORITHMS
FilteredBack Projection :
A traditional method that uses convolution filters to reduce blurring and reconstructs
images quickly.
It is used widely but can introduce noise and artifacts
Iterative Reconstruction :
A modern approach that starts with an initial image assumption and refines it through
multiple iterations.
It reduces noise and improves image quality while minimizing radiation dose.
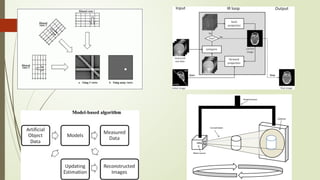
Model Based Iterative Reconstruction
A more advanced version of iterative reconstruction incorporating statistical modelling,
physics and optics
Provides superior image clarity and accuracy, esp in low dose scan
6.
Cone BeamReconstruction
These are specifically designed for cone beam CT scanners, this algorithm
processes data from multiple angels to create 3D images
Deep Learning Based Recontruction
Convolutional neural networks (CNNs), are trained on large datasets to learn
patterns and features in medical images. These models can reconstruct high-
quality images from raw or noisy data.
This newer cutting edge approach is currently gaining traction in modern CT
Imaging
8.
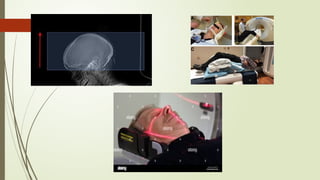
CT POSITIONING FORHEAD IMAGING
Patient positioning – patient lies supine on CT table with head placed in
headrest for stability, aligned in the midline, ensuring no tilt or rotation
The chin is slightly tucked to align the orbitomeatal line (OML)
perpendicular to the table
Landmark
External landmark – External auditory meatus and outer canthus of eye
Internal landmark – The base of skull and vertex
Location
Start – Base of skull (foramen magnum)
End – Vertex of skull
10.
CT POSITIONING INCERVICAL SPINE
Patient positioning – Patient lies supine with head, neck aligned to midline
Arms are positioned alongside body with shoulders pulled down
Landmarks
External – Sternal notch and external auditory meatus
Internal – Hyoid bone and thyroid cartilage
Locations
Start – Base of the skull to include upper cervical spine and pharynx
End – Extends to thoracic inlet covering lower spine
12.
CT POSITIONING INCHEST
Patient positioning – patient supine
Both arms raised above head to reduce interference in chest region
Landmarks
External – Sternal notch (manubrium) and xiphoid process
Internal – apex of lung and diaphragm level
Location
Start – Begins at apex of lung (just above thoracic inlet)
End – Extends to costophrenic angles (just below the diaphragm)
Patient is instructed to hold the breath to minimize motion artifacts
Confirm field of view (FOV) to ensure both lungs and mediastinum are incl.
15.
CT POSITIONING INABDOMEN
Patient positioning – Lies supine
Arms are placed overhead
Landmarks
External – xiphoid process (upper landmark) and pubic symphasis (lower
landmark)
Internal – Including liver, kidneys, pancreas, spleen, bowel loops
Scan Location
Start - Above dome of diaphragm
End – Extend iliac crest or pubic symphasis
17.
CT Angiography ofHead, Neck, Chest and Abdomen
CT Contrast Protocols
19.
Used forenhancing visibility of blood vessels, tissues and abnormalities
Primarily Iodinated contrast are used
Ionic – Diatriazoate, iothalamate, metrizoate
Non ionic – iohexol, iopamidol, iodixanol (Pref due to less ADR)
Osmolarity
High Osmolality – Older agents, high ADR
Low Osmolality – Newer agent, safer, widely used.
20.
What to tellthe patient before giving
contrast?
“Normal anatomy on CT Scan is all grey. Air shows up black, and bone
shows up bright white. Without any kind of contrast, All the blood vessels in
your brain will appear grey. The contrast agent will help to highlight the
blood vessels and any problems associated with it. It will also highlight any
kind of infection or inflammation or bleeding. So if there’s anything going on
in there, chances are, I’m going to be able to see it. The IV contrast will give
you a warm feeling all over, but sometimes it’ll vary from person to person. It
will also give you a little bit of a metal taste. This is all normal. Sometimes the
contrast will make people a little bit noxious, but if you have any kind of
problems, please, let me know. Do you have any questions?”
21.
Preparation for CTangio Patient
Fasting
Hydration
Medication Review
Contrast Allergy check
RFT (BUN and creatinine)
IV Placement
Comfortable clothing
Breath hold Practice
22.
Medication Review
BetaBlockers
Lower heart rate for better clarity esp for cardiac CT angiography
Nitroglycerine
Dilate coronary arteries, enhancing vessel visualization
AntiHistamine and Steroids
Premedicate in patients with contrast allergies to reduce reaction risk
Anticoagulants
Review to assess bleeding risk esp if invasive procedures are planned post
angiography
23.
Review of Metforminin CT
Angiography
Rare but serious risk of Metformin Associated Lactic Acidosis (MALA)
Mechanism :
Iodinated contrast can temporarily affect kidney function leading to reduced
clearance of metformin and accumulation of lactate which may trigger lactic
acidosis
Pre Procedure Guidelines:
Assess RFT by test like serum creatinine or GFR
Discontinue metformin 24 to 48 hours before producer if GFR < 30 ml/min/1.73 m2
Post Procedure Guidelines:
Reassess RFT 48 hours after procedure
Resume metformin only if RFT is stable and within normal limits
24.
Impact of breathholding on various
Imaging
Motion reduction
Minimize respiratory motion, prevents blurring and motion artifacts
Improved Clarity
Blood vessels and organs appear sharper and more defined
Accurate Alignment
Essential for studies like CT Angiography where precise timing with contrast
injection is critical
Patient Compliance
Provides consistent and reproducible imagine results
25.
When to captureImages?
After giving contrast through IV, it travels up the arm to the heart and then
to the brain and other organs. To catch the images we need to capture
contrast in its desired phase.
Usually this is during the venous phase as both veins and arteries have
contrast
Timing helps to capture the images at the right moment
26.
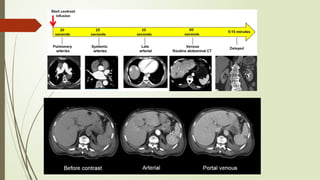
Phases of enhancement
The purpose of CECT is to find lesion which many be hypovascular or
hypervascular as compared to the normal tissue.
The various phases help in identifying and highlighting certain tissues which
take up or lose contrast as per its corresponding uptake.
27.
Non-enhanced CT
• Detectionof calcifications, fat in tumors, fat stranding in inflammations like appendicitis,
diverticulitis
Early arterial phase
• Contrast is still in arteries and has not enhanced organs or soft tissues
Late arterial phase
• Structures receiving blood supply will show optimal enhancement
Hepatic or late portal phase
• Liver parenchyma enhances through portal vein blood supply
Nephrogenic phase
• All of renal parenchyma enhances including medulla enhances.
Delayed phase
• Wash out of contrast in abdominal structures except for fibrotic tissue
Hounsfield Units
HounsfieldUnits (HU) are a scale used in CT imaging to measure tissue
density relative to water.
Water is assigned 0 HU, air is -1000 HU, and dense structures like bone range
up to +1000 HU or more. Different tissues have specific HU values, aiding in
differentiation.
The human eye can only differentiate upto 20 shades of grey effectively
CT images contain upto 256 shades of grey which make it difficult for
interpretation of CT images
32.
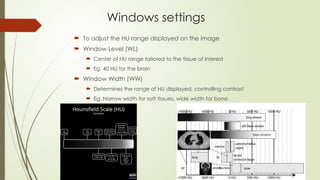
Windows settings
Toadjust the HU range displayed on the image
Window Level (WL)
Center of HU range tailored to the tissue of interest
Eg. 40 HU for the brain
Window Width (WW)
Determines the range of HU displayed, controlling contrast
Eg. Narrow width for soft tissues, wide width for bone
33.
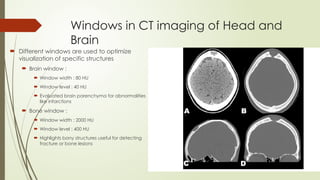
Windows in CTimaging of Head and
Brain
Different windows are used to optimize
visualization of specific structures
Brain window :
Window width : 80 HU
Window level : 40 HU
Evaluated brain parenchyma for abnormalities
like infarctions
Bone window :
Window width : 2000 HU
Window level : 400 HU
Highlights bony structures useful for detecting
fracture or bone lesions
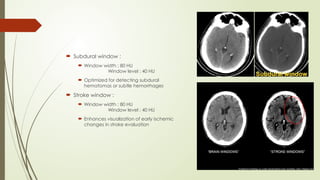
34.
Subdural window:
Window width : 80 HU
Window level : 40 HU
Optimized for detecting subdural
hematomas or subtle hemorrhages
Stroke window :
Window width : 80 HU
Window level : 40 HU
Enhances visualization of early ischemic
changes in stroke evaluation
35.
CT Positioning inHead with Contrast
Position / Landmark Center on patient’s chin
Scan Start Below base of skull (foramen magnum)
Scan End Vertex of the skull
Breath Hold None
IV Access 22 G or larger, antecubital
IV Contrast Adult 100 ml OMNI 300 @ 2.0mL/ sec
Contrast Delay Scan 5 minutes from Start of Injection
36.
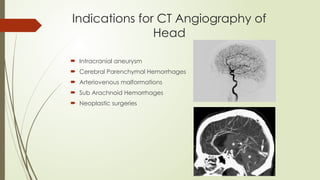
Indications for CTAngiography of
Head
Intracranial aneurysm
Cerebral Parenchymal Hemorrhages
Arteriovenous malformations
Sub Arachnoid Hemorrhages
Neoplastic surgeries
37.
CT Angiography Headand Neck
Position / Landmark Level of Aortic Arch
Scan Start Below Aortic Arch
Scan End Above Skull
Breath hold None
IV Access 20 G or larger, Antecubital
IV Contrast Adults 50 ml OMNI 350 @ 5.0 ml/sec
Contrast Delay Bolus Tracked : Trigger Scan @ 120 HU
38.
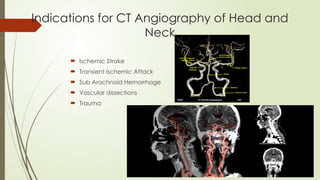
Indications for CTAngiography of Head and
Neck
Ischemic Stroke
Transient Ischemic Attack
Sub Arachnoid Hemorrhage
Vascular dissections
Trauma
39.
CT positioning inChest with Contrast
Position / Landmark Supine centered above the lung
apices
Scout Scan Start Above lung apices
Scout Scan End Adrenals / upper kidneys
Breath hold Inspiration
IV Access 18G -22G
Location: No lower than 2” below the
AC crease of the elbow, pressure
approved TLC, PICC lines,
(NOTE: For PV IV flush with the arm in
the position it will be for the scan)
IV Contrast Adults OMNI 350 80 ml
Contrast Delay 60 sec
40.
Indications for CECT Chest
Suspected cases of lung cancer and staging
purposes
Thoracic vascular diseases
Pulmonary Parenchymal diseases
Pleural diseases
Airway evaluation
Sternal and Mediastinal infections
41.
ADR associated toContrast
Idiosynscratic reactions
Mild : scattered urticarial rashes, pruritis, retching,
Moderate : Vomiting, facial edema, tachycardia
Severe : arrhythmias, laryngeal edema, pulmonary edema, seizures
Nonidiosyncratic reactions :
Mostly due heightened sympathetic activity : bradycardia, hypotension, and
vasovagal reactions; neuropathy; cardiovascular reactions; extravasation; and
delayed reactions.
Other nonidiosyncratic reactions include sensations of warmth, a metallic taste in
the mouth, and nausea and vomiting.
42.
Management of ADRin CECT
For any reactions : STOP CONTRAST ADMINISTRATION
Depending upon severity of the reaction (One or more steps to be followed):
Call for help
Airway , Breathing, Circulation
Epinephrine Administration ( 0.3 – 0.5 mg )
Antihistamines : Inj Chlorpheniramine maleate (25 -50 mg)
Corticosteroids : Inj Hydrocortisone (100 mg)
Bronchodilators : B2 agoinst
IV Fluids
Monitor, document and follow up
43.
Specific ADR
Nephropathy:
Elevation of 0.5 mg% or more than baseline of creatinine after 1-3 days after
ICM injections. The elevation reaches peak by 7 days and returns to normal
by 14 days.
Incidence is estimated around 2-7 % of population.
Post sequelae of is persistent decrease of renal function in upto 25% patients
Cardiovascular reactions :
Due to vasovagal reactions due to anaphylactic reactions
Bradycardia with peripheral vasodilation with lower threshold for ventricular
arrhythmias and cardiac arrest in severe cases.
Majority cases are self limiting but can be an indicator of a more severe
evolving reactions
44.
Management of Contrastassociated Nephropathy
Monitor RFT
Supportive care : Provide fluids to maintain hydration and kidney function
Dialysis in severe case
Renal Replacement therapy
Avoid further contrast exposure