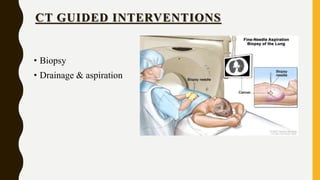
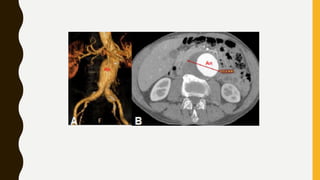
CT scan uses X-rays and computers to create detailed images of the inside of the body. It has replaced conventional angiography as the primary method for examining blood vessels. The document discusses the history, components, principles, types (including spiral, multidetector, angiography), advantages, and risks of CT scanning. CT guided procedures such as biopsy and drainage are also summarized.





































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)