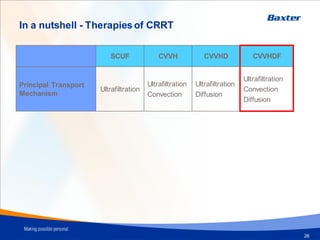
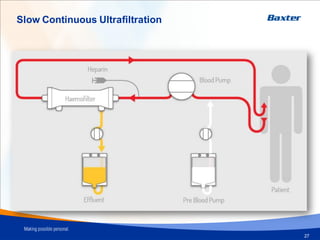
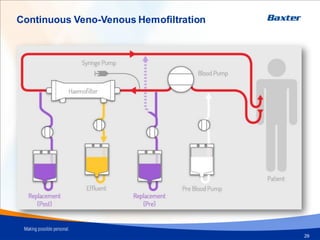
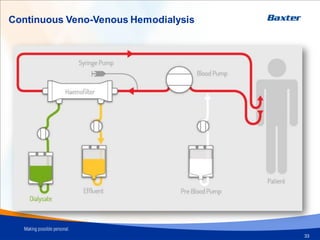
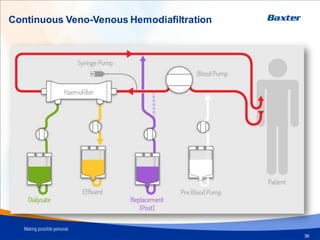
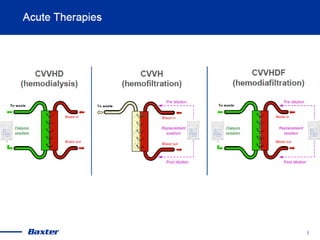
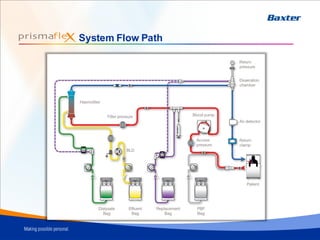
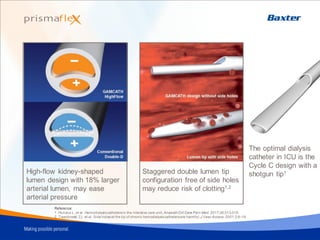
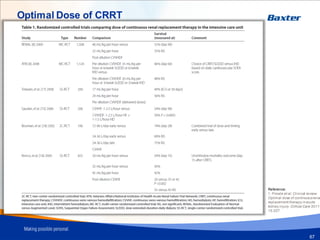
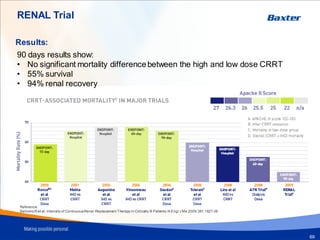
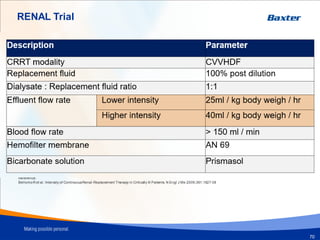
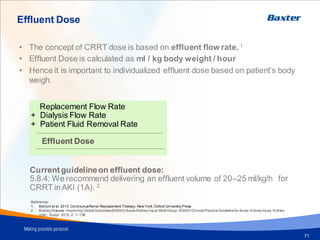
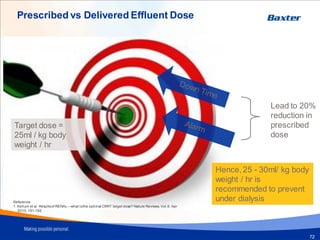
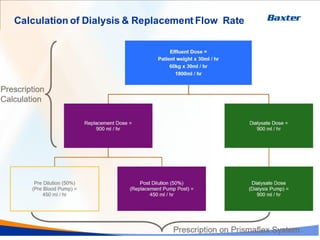
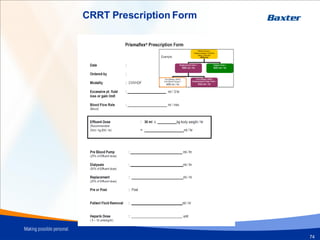
Continuous renal replacement therapy (CRRT) modalities include slow continuous ultrafiltration (SCUF), continuous veno-venous hemofiltration (CVVH), continuous veno-venous hemodialysis (CVVHD), and continuous veno-venous hemodiafiltration (CVVHDF). The Prismaflex system provides a user-friendly platform for individualized CRRT prescriptions using various components like filters, solutions, and catheters. Optimal CRRT dosing is recommended at 20-25 ml/kg/hr based on studies showing no significant difference in mortality between high and low intensity doses in that range.




























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

