2
Introduction
• Acute kidneyinjury (AKI) is a common complication in critically ill patients and is
associated with substantial morbidity and risk of death
• Approximately 5% to 10% of patients with AKI require renal replacement therapy
(RRT) during their ICU stay1
• Mortality rates of 30% to 70%.2-4
• Over the past 2 decades, the incidence of RRT requiring AKI has increased by
approximately 10% per year5
1. Tolwani A. Continuous renal-replacement therapy for acute kidney injury. N Engl J Med. 2012;367(26):2505-2514
2. Tandukar, S; Palevsky, P; Continuous Renal Replacement Therapy Who, When, Why, and How Chest 2019 Mar;155(3):626-638
3.
Introduction
• Continuous renalreplacement therapy (CRRT) is commonly used to provide renal
support for critically ill patients with acute kidney injury, particularly patients who
are hemodynamically unstable1
• A variety of techniques that differ in their mode of solute clearance may be used1
• However, substantial uncertainty remains regarding many of the fundamental
aspects of RRT management1
• As with other dialysis techniques, CRRT requires a well-functioning access, a
permeable membrane, pumps to circulate blood and various solutions across
the membrane with accurate fluid balancing, and pressure monitoring systems. 2
1.Tadunkar, S.; Palevsky P., Continuous Renal Replacement Therapy Who, When, Why, and How CHEST 2019; 155(3):626-638
2. Macedo, E.;Mehta R, Am J Kidney Dis. Continuous Dialysis Therapies: Core Curriculum 2016;2016;68(4):645-657
4.
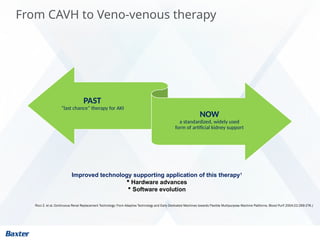
From CAVH toVeno-venous therapy
Ricci Z. et al, Continuous Renal Replacement Technology: From Adaptive Technology and Early Dedicated Machines towards Flexible Multipurpose Machine Platforms. Blood Purif 2004;22:269-276.|
PAST
“last chance” therapy for AKI
NOW
a standardized, widely used
form of artificial kidney support
Improved technology supporting application of this therapy1
Hardware advances
Software evolution
5.
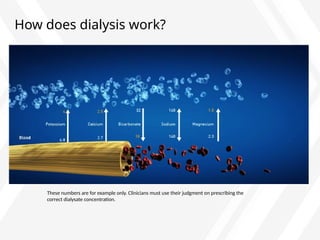
Solute clearance andmodality selection
As in the glomerulus,
removal of fluid and solutes
in CRRT occurs through
a semi-permeable
membrane
This concept is known as selective
permeability, meaning that certain substances
will cross the membrane and others will not be
allowed to cross
8
Basic components ofCRRT
Baxter Confidential — Do not distribute without prior approval |
CRRT
Hemofilt
er
Vascu
lar
Acces
s
Anticoagula
tion
Solutio
ns
Blood
Warm
er
CRRT
Syste
m
9.
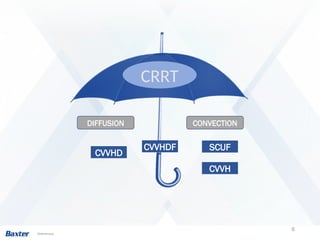
CRRT Treatment Modalities:
ContinuousVenovenous Hemodialysis (CVVHD)
Rona A, Fumagalli R. Indications for Renal Replacement Therapy in the Critically Ill Patient. In: Critical Care Nephrology; 2nd ed. Philadelphia, PA: Saunders Elsevier; 2009:1328-1332
Primary Therapeutic Goal:
• Safe fluid removal and solute
clearance
Principles Used:
• Diffusion
Therapy Characteristics:
Requires dialysate to drive diffusion
No replacement fluid
Used to achieve solute removal (small and
medium sized molecules) and fluid balance
Blood flow variable
Primary Indications:
• Uremia, acid/base or electrolyte
imbalance, fluid overload
10.
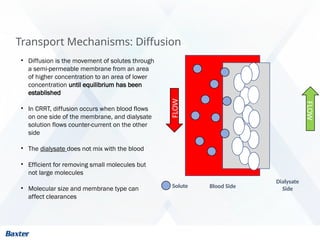
Transport Mechanisms: Diffusion
•Diffusion is the movement of solutes through
a semi-permeable membrane from an area
of higher concentration to an area of lower
concentration until equilibrium has been
established
• In CRRT, diffusion occurs when blood flows
on one side of the membrane, and dialysate
solution flows counter-current on the other
side
• The dialysate does not mix with the blood
• Efficient for removing small molecules but
not large molecules
• Molecular size and membrane type can
affect clearances
FLOW
Blood Side
Dialysate
Side
Solute
FLOW
11.
Transport Mechanisms: Diffusion
•Solute transfer across the membrane
occurs by movement down a
concentration gradient from blood to
dialysate until equilibrium has been
established 1
• Lower molecular weight (< 500-1,500
Daltons) solutes (smaller circles)
cross the membrane more readily
than higher molecular weight solutes
(larger circles)1
FLOW
Blood Side
Dialysate
Side
FLOW
Solutes
1. Tandukar, Srijan et al. Continuous Renal Replacement Therapy CHEST, March 2019 Volume 155, Issue3, Pages 626–638
12.
CRRT Treatment Modalities:
ContinuousVenovenous Hemodialysis (CVVHD)
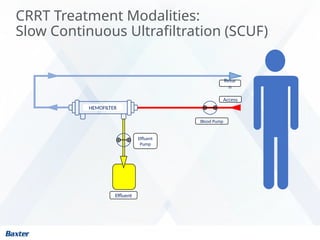
Blood Pump
Effluent
Dialysate
Retur
n
Access
Effluent
Pump
HEMOFILTER
Dialysi
s
Pump
13.
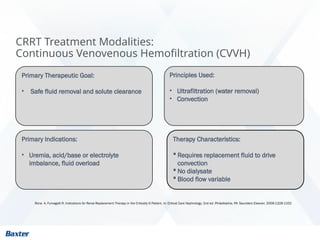
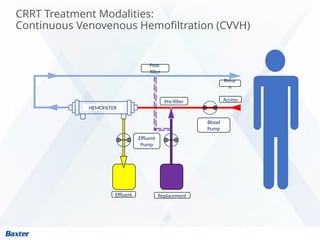
CRRT Treatment Modalities:
ContinuousVenovenous Hemofiltration (CVVH)
Rona A, Fumagalli R. Indications for Renal Replacement Therapy in the Critically Ill Patient. In: Critical Care Nephrology; 2nd ed. Philadelphia, PA: Saunders Elsevier; 2009:1328-1332
Primary Therapeutic Goal:
• Safe fluid removal and solute clearance
Principles Used:
• Ultrafiltration (water removal)
• Convection
Therapy Characteristics:
Requires replacement fluid to drive
convection
No dialysate
Blood flow variable
Primary Indications:
• Uremia, acid/base or electrolyte
imbalance, fluid overload
14.
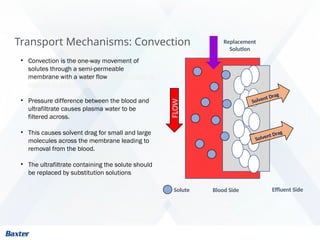
Transport Mechanisms: Convection
SolventDrag
• Convection is the one-way movement of
solutes through a semi-permeable
membrane with a water flow. Sometimes it is
referred to as solvent drag
• Pressure difference between the blood and
ultrafiltrate causes plasma water to be
filtered across.
• This causes solvent drag for small and large
molecules across the membrane leading to
removal from the blood.
• The ultrafiltrate containing the solute should
be replaced by substitution solutions
Solvent Drag
Blood Side Effluent Side
FLOW
Solute
Replacement
Solution
15.
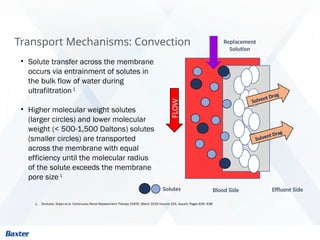
Transport Mechanisms: Convection
SolventDrag
• Solute transfer across the membrane
occurs via entrainment of solutes in
the bulk flow of water during
ultrafiltration1
• Higher molecular weight solutes
(larger circles) and lower molecular
weight (< 500-1,500 Daltons) solutes
(smaller circles) are transported
across the membrane with equal
efficiency until the molecular radius
of the solute exceeds the membrane
pore size1
Solvent Drag
Blood Side Effluent Side
FLOW
Replacement
Solution
Solutes
1. Tandukar, Srijan et al. Continuous Renal Replacement Therapy CHEST, March 2019 Volume 155, Issue3, Pages 626–638
17
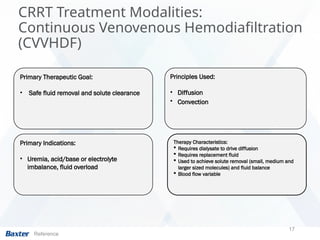
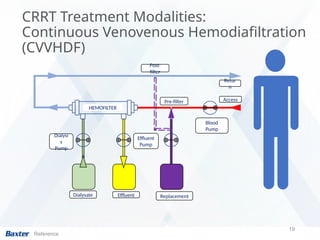
CRRT Treatment Modalities:
ContinuousVenovenous Hemodiafiltration
(CVVHDF)
Reference
Primary Therapeutic Goal:
• Safe fluid removal and solute clearance
Principles Used:
• Diffusion
• Convection
Therapy Characteristics:
Requires dialysate to drive diffusion
Requires replacement fluid
Used to achieve solute removal (small, medium and
larger sized molecules) and fluid balance
Blood flow variable
Primary Indications:
• Uremia, acid/base or electrolyte
imbalance, fluid overload
18.
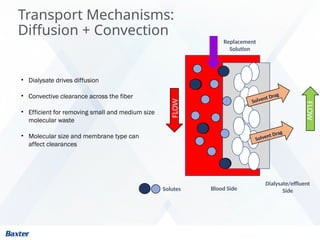
Transport Mechanisms:
Diffusion +Convection
• Dialysate drives diffusion
• Convective clearance across the fiber
• Efficient for removing small and medium size
molecular waste
• Molecular size and membrane type can
affect clearances
FLOW
Blood Side
Dialysate/effluent
Side
FLOW
Solvent Drag
Solvent Drag
Replacement
Solution
Solutes
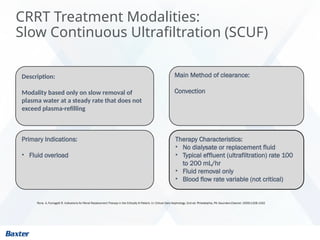
CRRT Treatment Modalities:
SlowContinuous Ultrafiltration (SCUF)
Rona A, Fumagalli R. Indications for Renal Replacement Therapy in the Critically Ill Patient. In: Critical Care Nephrology; 2nd ed. Philadelphia, PA: Saunders Elsevier; 2009:1328-1332
Description:
Modality based only on slow removal of
plasma water at a steady rate that does not
exceed plasma-refilling
Main Method of clearance:
Convection
Therapy Characteristics:
• No dialysate or replacement fluid
• Typical effluent (ultrafiltration) rate 100
to 200 mL/hr
• Fluid removal only
• Blood flow rate variable (not critical)
Primary Indications:
• Fluid overload
21.
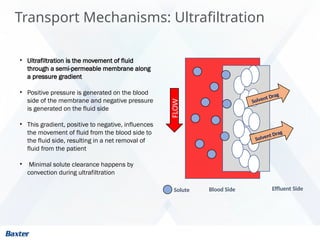
Transport Mechanisms: Ultrafiltration
SolventDrag
• Ultrafiltration is the movement of fluid
through a semi-permeable membrane along
a pressure gradient
• Positive pressure is generated on the blood
side of the membrane and negative pressure
is generated on the fluid side
• This gradient, positive to negative, influences
the movement of fluid from the blood side to
the fluid side, resulting in a net removal of
fluid from the patient
• Minimal solute clearance happens by
convection during ultrafiltration
Solvent Drag
Blood Side Effluent Side
FLOW
Solute
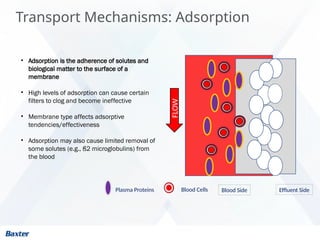
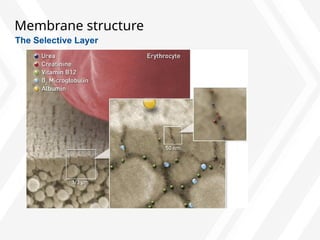
Transport Mechanisms: Adsorption
•Adsorption is the adherence of solutes and
biological matter to the surface of a
membrane
• High levels of adsorption can cause certain
filters to clog and become ineffective
• Membrane type affects adsorptive
tendencies/effectiveness
• Adsorption may also cause limited removal of
some solutes (e.g., ß2 microglobulins) from
the blood
Effluent Side
Blood Side
Plasma Proteins Blood Cells
FLOW
24.
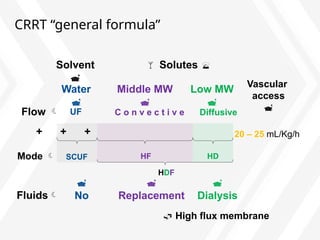
CRRT “general formula”
++ + 20 – 25 mL/Kg/h
HD
SCUF HF
HDF
Flow C o n v e c t i v e Diffusive
UF
Water
Middle MW
Low MW
Solutes
Solvent
Mode
High flux membrane
No
Replacement
Dialysis
Fluids
Vascular
access
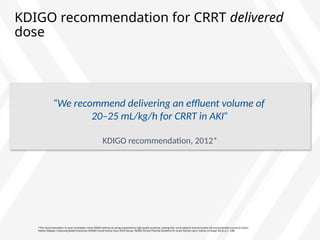
KDIGO recommendation forCRRT delivered
dose
*This recommendation is Level 1A Graded, which KDIGO defines as being supported by high-quality evidence, stating that ‘most patients should receive the recommended course of action’
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012;2:1–138.
“We recommend delivering an effluent volume of
20–25 mL/kg/h for CRRT in AKI”
KDIGO recommendation, 2012*
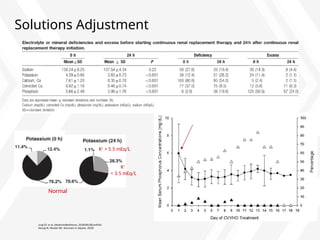
27.
How can thedifference between prescribed
and delivered dose be addressed?
*This recommendation is ‘Not graded’, which KDIGO defines as “used, typically, to provide guidance based on common sense or where the topic
does not allow adequate application of evidence”
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury.
Kidney Int Suppl 2012;2:1–138.
“In clinical practice, in order to achieve a delivered dose of
20–25 mL/kg/h, it is generally necessary to prescribe in the range of
25–30 mL/kg/h, and to minimize interruptions in CRRT”
KDIGO, 2012
*
28.
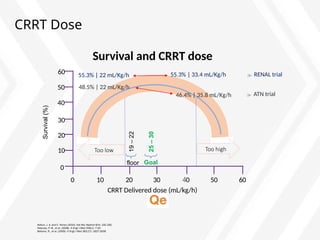
CRRT Dose
0
10
20
30
40
50
60
10 2030 40 50 60
0
Kellum, J. A. and C. Ronco (2010). Nat Rev Nephrol 6(4): 191-192.
Palevsky, P. M., et al. (2008). N Engl J Med 359(1): 7-20.
Bellomo, R., et al. (2009). N Engl J Med 361(17): 1627-1638.
CRRT Delivered dose (mL/kg/h)
Survival
(%)
Too low Too high
RENAL trial
55.3% | 22 mL/Kg/h 55.3% | 33.4 mL/Kg/h
ATN trial
48.5% | 22 mL/Kg/h
46.4% | 35.8 mL/Kg/h
floor
19
–
22
25
–
30
Goal
Survival and CRRT dose
29.
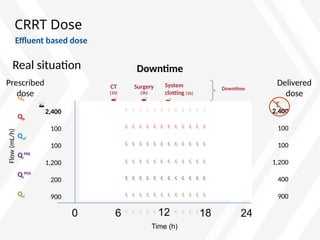
CRRT Dose
Real situationDowntime
Effluent based dose
0 24
12
Time (h)
2,400
100
100
1,200
400
900
6 18
CT
(1h)
Surgery
(3h)
System
clotting (1h)
Downtime
Prescribed
dose
Qe
Qb
Quf
Qr
PRE
Qr
POS
Qd
2,400
100
100
1,200
200
900
Flow
(mL/h)
Delivered
dose
30.
CRRT Prescription
• TheKDIGO Clinical Practice Guideline recommends the following preferences for
choosing a vein for insertion of a dialysis catheter in patients with AKI:
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury.
Kidney Int Suppl 2012;2:1–138.
Section 5.4.2 (Not graded):
− First choice: right jugular vein (12 -15 cm)
− Second choice: femoral vein (19 – 24 cm)
− Third choice: left jugular vein (15 – 20 cm)
− Last choice: subclavian vein with preference for the dominant side
A functional vascular access is the key to a successful CRRT
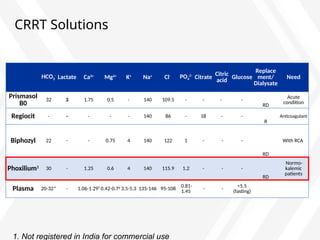
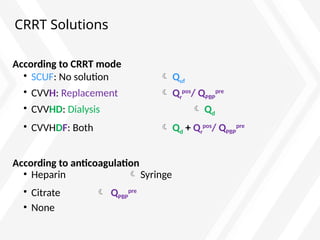
CRRT Solutions
According toCRRT mode
• SCUF: No solution Quf
• CVVH: Replacement Qr
pos
/ QPBP
pre
• CVVHD: Dialysis Qd
• CVVHDF: Both Qd + Qr
pos
/ QPBP
pre
According to anticoagulation
• Heparin Syringe
• Citrate QPBP
pre
• None
46.
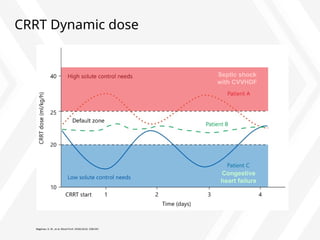
CRRT Dynamic dose
Bagshaw,S. M., et al. Blood Purif. 2016;42(3): 238-247.
Septic shock
with CVVHDF
Congestive
heart failure
Editor's Notes
#27 Figure on right:
Patients at risk of cerebral edema who require RRT will benefit from therapies that have less impact on osmolar shifts to maintain intracranial pressure.
Figure (left) adapted with permission from Kellum, et al. Continuous Renal Replacement Therapy. New York, NY. Oxford University Press. 2010; p 58.
Figure (right) adapted with permission from Davenport. Am J Kidney Dis. 2003;3:457–466.
#29 Reference
1. Neri M, et al. Crit Care. 2016;20:318.
2. Villa G, et al. Contrib Nephrol. 2018;194:38-50.
3. Ronco C, et al. Lancet. 2000;356:26-30.
4. Claure-Del Granado R, Mehta RL. Semin Dial. 2011;24:157-63.
#30 Reference
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012;2:1–138.
#31 Reference
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012;2:1–138.
#32 Reference
Kellum, J. A. and C. Ronco (2010). Nat Rev Nephrol 6(4): 191-192.
Palevsky, P. M., et al. (2008). N Engl J Med 359(1): 7-20.
Bellomo, R., et al. (2009). N Engl J Med 361(17): 1627-1638.
#35 Reference
Vijayan, A. (2009). Semin Dial 22(2): 133-136.
Engstrom, B. I., et al. (2013). J Vasc Interv Radiol, 24(9), 1295-1302.
KDIGO Clinical Practice Guideline for Acute Kidney Injury." Kidney International Supplements 2(1): 89-115.
#38 Reference
Fealy, N., et al. (2018). Crit Care Resusc 20(1): 41-47.
#39 Reference
Rosner, M. H., et al. (2014). Br J Anaesth 113(5): 764-771.
Hoste, E. A., et al. (2014). Br J Anaesth 113(5): 740-747.
#40 Reference
Rosner, M. H., et al. (2014). Br J Anaesth 113(5): 764-771.
O'Connor, M. E. and J. R. Prowle (2015). "Fluid Overload." Crit Care Clin 31(4): 803-821.
#51 Reference
Continuous Renal Replacement Therapy, (2010) Kellum, Bellomo, (pp.11-13) Ronco, New York, USA Oxford University Press
Baldwin, I. Nonanticoagulation strategies to optimize circuit function in renal replacement therapy (pp.129-134) Bellomo, R & Baldwin, I. Anticoagulation (pp. 135-140) Fealy, N. Regional citrate anticoagulation (pp.141-146) In J.A. Kellum, R. Bellomo & C. Ronco (Eds) Continuous Renal Replacement Therapy, (2010) New York, USA Oxford University Press
#55 Reference
1. Bagshaw, S. M., et al. Blood Purif. 2016;42(3): 238-247.









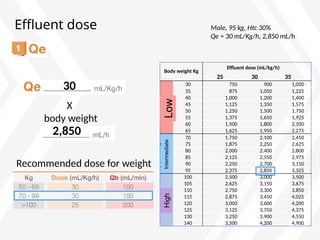


![Effect of predilution on CRRT dose
CRRT Downtime
0 24
12
Time (h)
1,968
(20 mL/kg/h)
6 18
Prescribed
dose
Delivered
dose
(26 mL/kg/h)
Dilution
correction
Downtime
adjustment
(24 – 5 = 19h)
Flow
(mL/h)
2,565
CT
(1h)
Surgery
(3h)
System
clotting (1h)
Downtime
1 + 3 + 1 = 5h
2,565
Qe
Prescribed dose ≠ Delivered dose
2,850
(30 mL/kg/h)
2,850
(30 mL/kg/h)
Average dose
(2,486 mL/h x 19h) + (0 mL/h x 5h)
24h
150
100
1,200
315
1,175
Qb
Quf
Qr
PRE
Qr
POS
Qd
Weight: 95 Kg, Hto 30%
Dilution factor:
(6,300/[6,300+1,260] = 0.83)
Dose correction for dilution:
0.83 x [100+1,260+315] + 1175 = 2,565 mL/h](https://image.slidesharecdn.com/doc-20221115-wa0003-250727115411-f8579740/85/DOC-20221115-WA0003-data-analytics-tool-pptx-36-320.jpg)
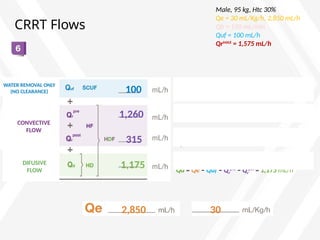
![CRRT flows: adjustment
30
2,850
Male, 95 kg, Htc 30%
Qe = 30 mL/Kg/h, 2,850 mL/h
Qb = 150 mL/min
Quf = 100 mL/h
QrMAX
= 1,575 mL/h
2,565 mL/h Qeadjusted [(0.83x(100+1260+315)) + 1175]
2,850 mL/h Qe unadjusted
–
285 mL/h
1,175
+ 285
1,460
+
1,460 mL/h](https://image.slidesharecdn.com/doc-20221115-wa0003-250727115411-f8579740/85/DOC-20221115-WA0003-data-analytics-tool-pptx-37-320.jpg)





























![[DSC Europe 25] Gordana Milutinovic Dumbelovic - From Insight to Oversight: A...](https://cdn.slidesharecdn.com/ss_thumbnails/t7dkjsfxqwwzceropjv4-gordana-milutinovicdumbelovic-from-insight-to-oversight-ai-driven-power-bi-moni-260119121559-9e0bf11b-thumbnail.jpg?width=640&height=640&fit=bounds)
![[DSC Europe 25] Harshvardhan Jain - From Pre-Trained to Purpose-Built: Fine-T...](https://cdn.slidesharecdn.com/ss_thumbnails/zru4zmiseku5tgvu2dgw-harshvardhan-jain-from-pre-trained-to-purpose-built-fine-tuning-llms-for-high-i-260119101520-8335585f-thumbnail.jpg?width=640&height=640&fit=bounds)

![[DSC Europe 25] Jovan Sumarac - Real-World Applications of Computer Vision in...](https://cdn.slidesharecdn.com/ss_thumbnails/fiksms22smcpopvvld03-jovan-sumarac-real-life-applications-of-computer-vision-in-automotive-systems-260120105855-de622abb-thumbnail.jpg?width=640&height=640&fit=bounds)
![[DSC Europe 25] Laila Kakar - Leveraging AI for Strategic Excellence: Enhanci...](https://cdn.slidesharecdn.com/ss_thumbnails/eykmhrtsqmaaftwkexh7-dsc-lailakakar-1-260119101520-5f3b5616-thumbnail.jpg?width=640&height=640&fit=bounds)













![[DSC Europe 25] Borko Kozomora - Optimizing business workflows with advances ...](https://cdn.slidesharecdn.com/ss_thumbnails/hbgekyb0txw0xpo4yfml-borko-kozomora-leading-ai-transformation-260122103838-cc29ee38-thumbnail.jpg?width=640&height=640&fit=bounds)
![[DSC Europe 25] Milovan Jovicic - Beyond AI's Reach: The Enduring Value of Ev...](https://cdn.slidesharecdn.com/ss_thumbnails/pyeij0hurgwq5jugmtnv-2-milovan-jovicic-beyond-ais-reach-the-enduring-value-of-evergreen-design-v2-260120105856-d6ee57e5-thumbnail.jpg?width=640&height=640&fit=bounds)