This document provides information about examining and affecting various cranial nerves. It discusses:
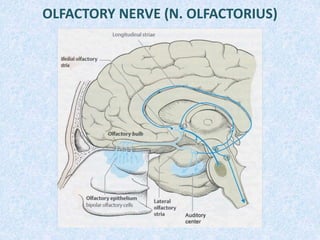
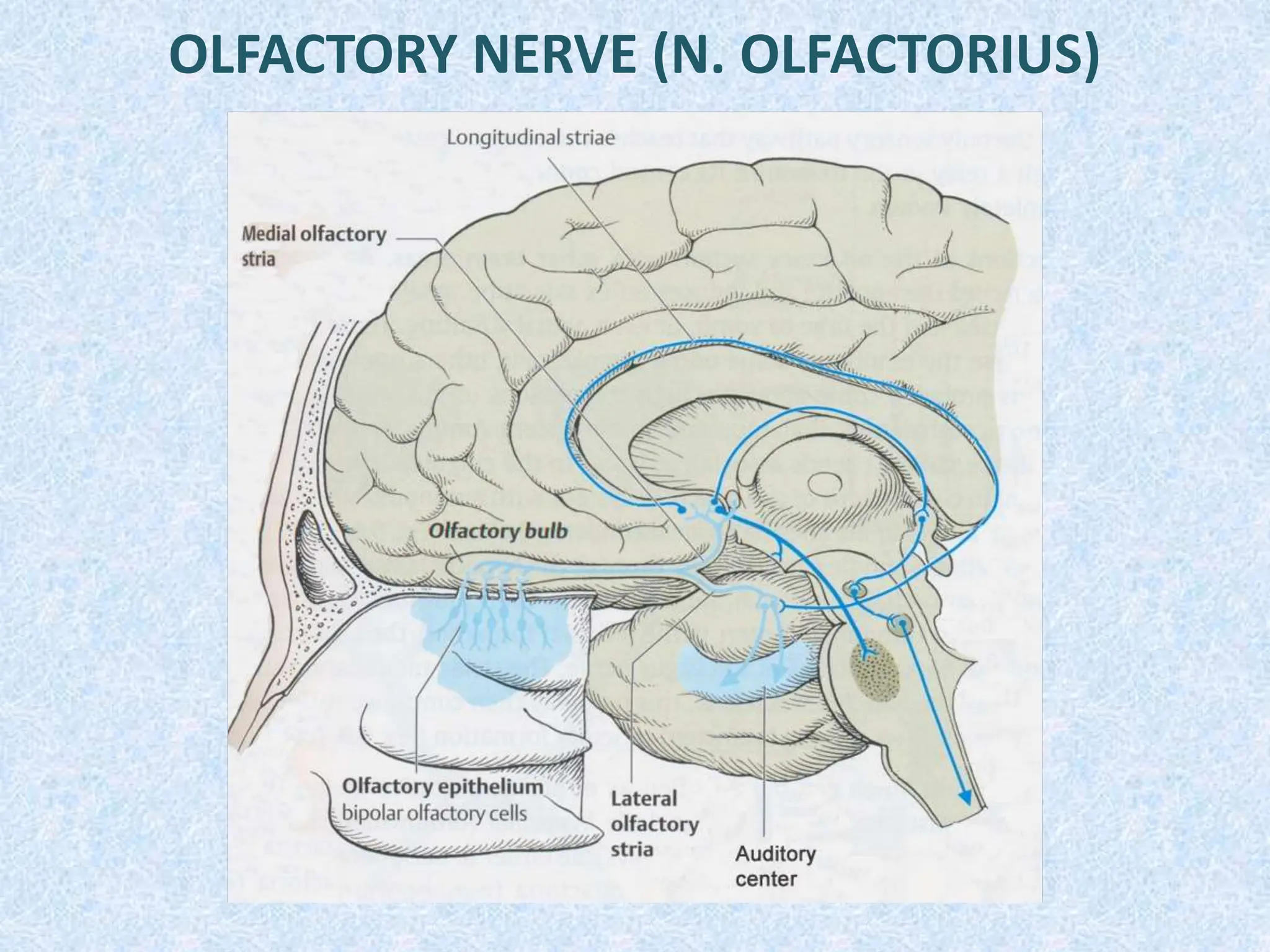
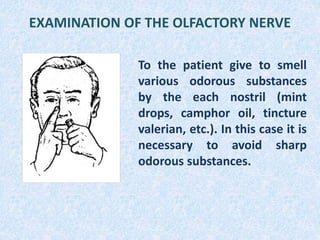
- Examining the olfactory nerve by having patients smell different odors. Dysfunctions of smell include hyposmia and anosmia.
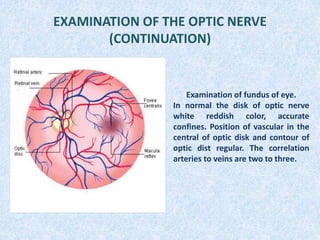
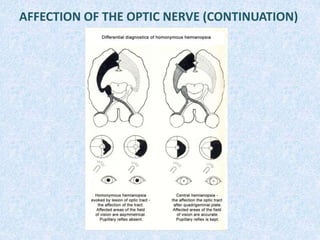
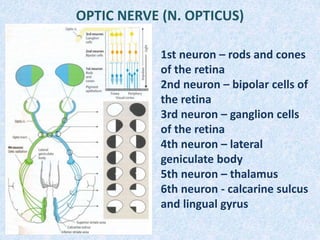
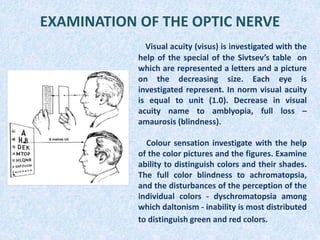
- Examining the optic nerve including visual acuity, color sensation, and visual fields. Affections can cause hemianopsias.
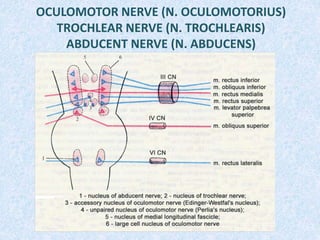
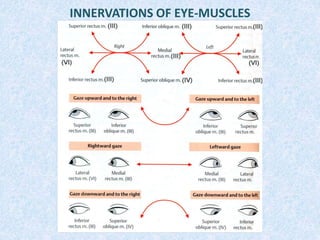
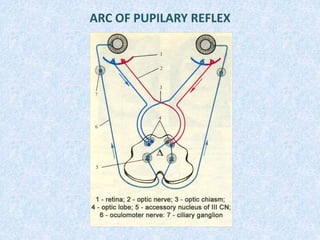
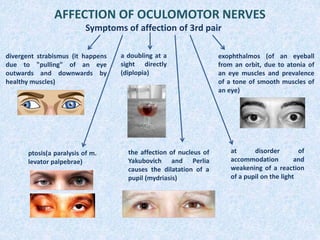
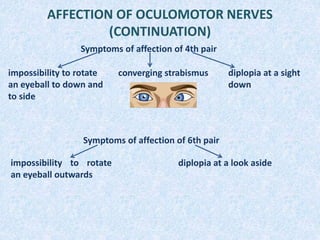
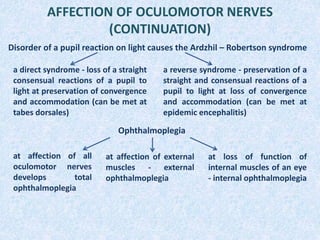
- Examining the oculomotor, trochlear and abducens nerves including eye movements and pupil reactions. Paralyses cause specific ophthalmoplegias.
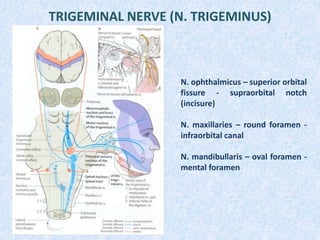
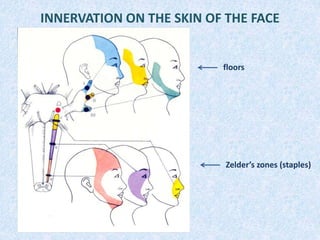
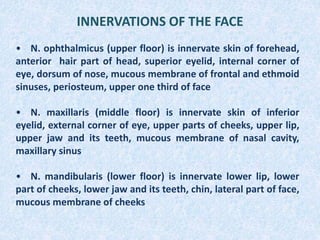
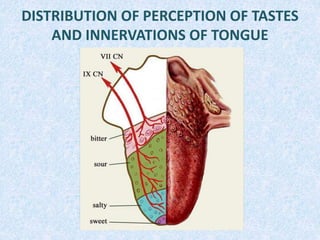
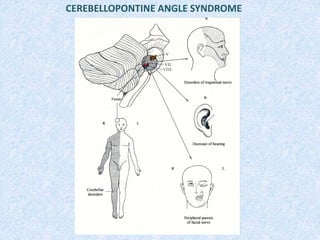
- Examining the trigeminal nerve includes sensitivity and reflexes. Affections cause sensory losses or neuralgias in innervation
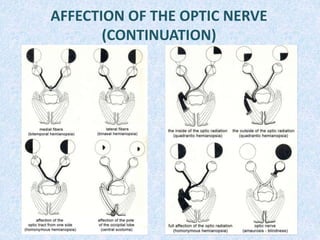
![Hemianopsia
Homonymous [(equi)lateral]
hemianopsia
Heteronymous [crossed]
hemianopsia
bitemporal
hemianopsia
binasal
hemianopsia
Quadrantic hemianopsia](https://image.slidesharecdn.com/cranialnerves-240101072728-5956cb99/85/cranial-nerves-ppt-7-320.jpg)