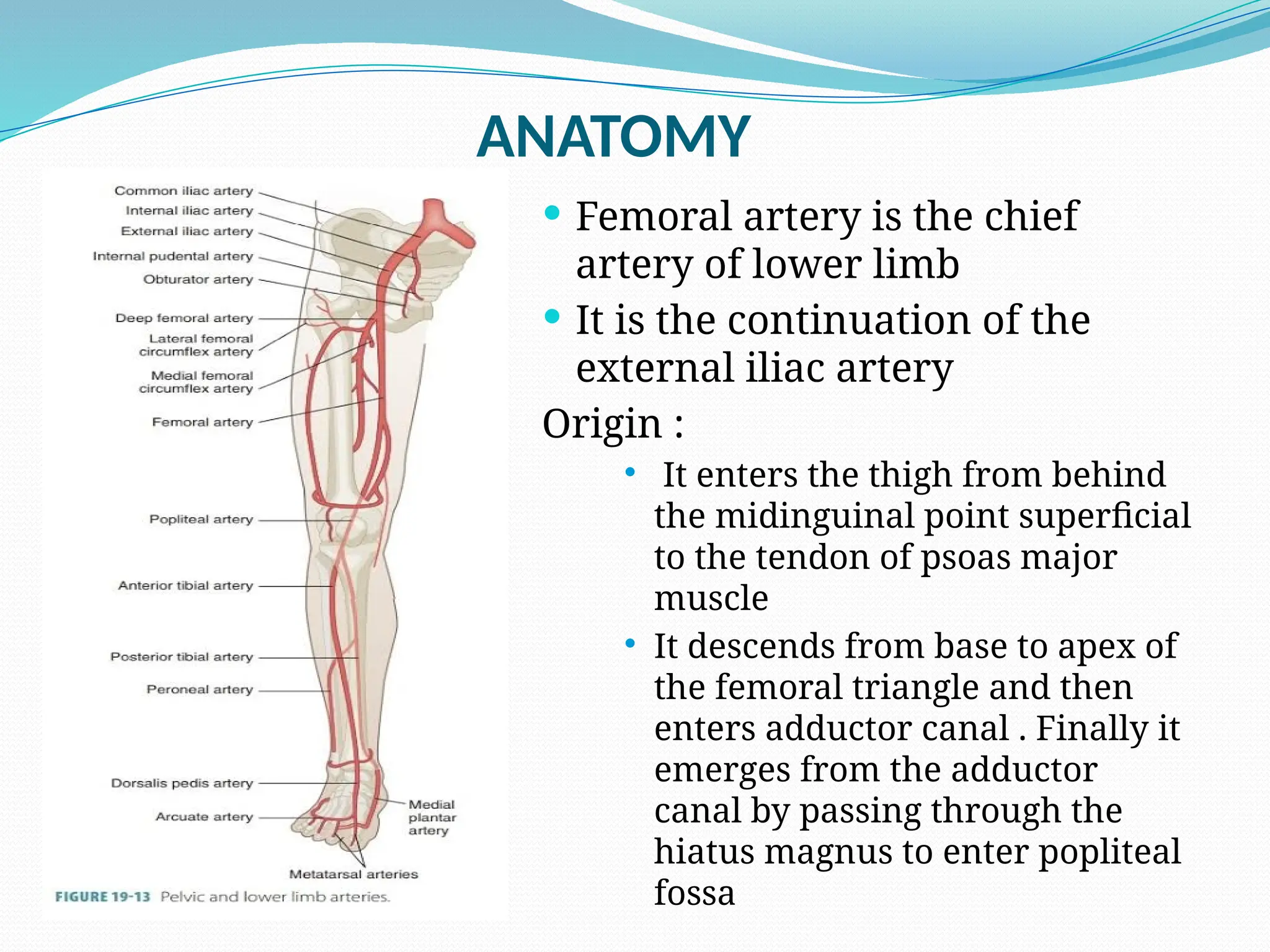
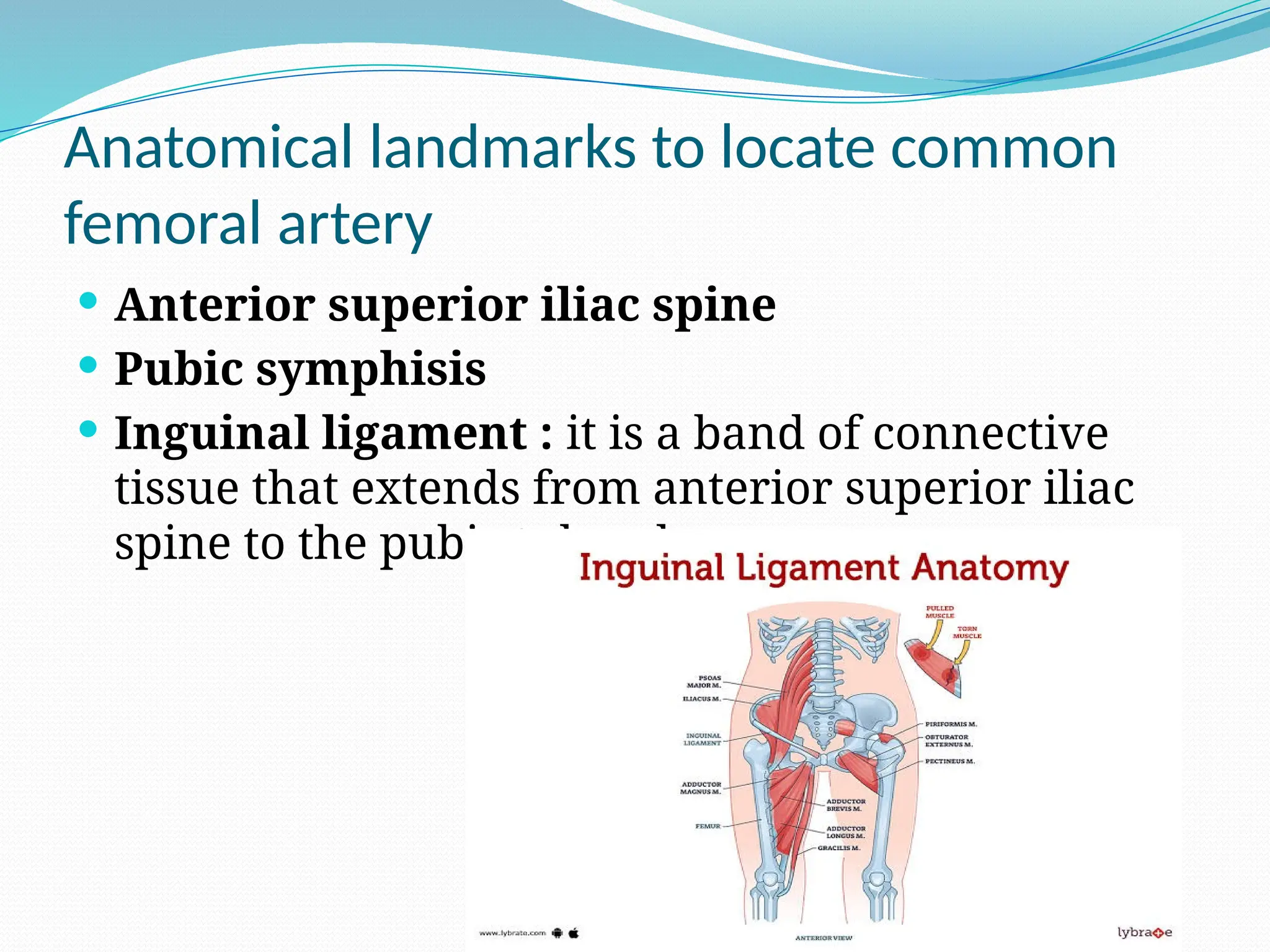
The document provides a detailed overview of femoral artery anatomy, access techniques, and associated complications related to cardiac catheterization. It outlines the anatomical landmarks for locating the common femoral artery, precise puncture techniques, and procedural steps for angiography. Additionally, it discusses the advantages, disadvantages, contraindications, and major complications, including retroperitoneal bleeding and pseudoaneurysm formation.



















































![Invasive_Cardio-Devices_procedures[1].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/invasivecardio-devicesprocedures1-240129085722-eb86cfb0-thumbnail.jpg?width=640&height=640&fit=bounds)





























