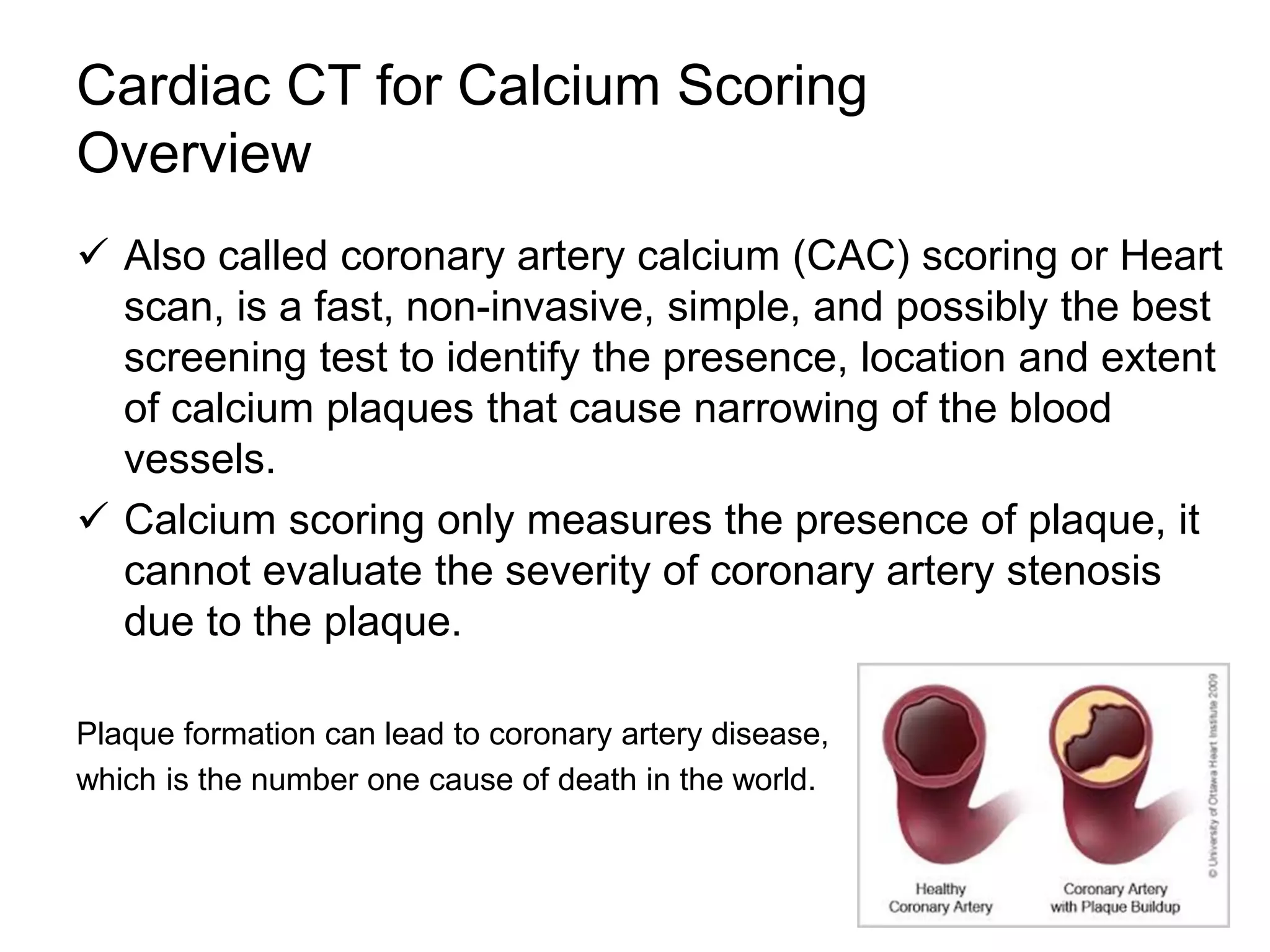
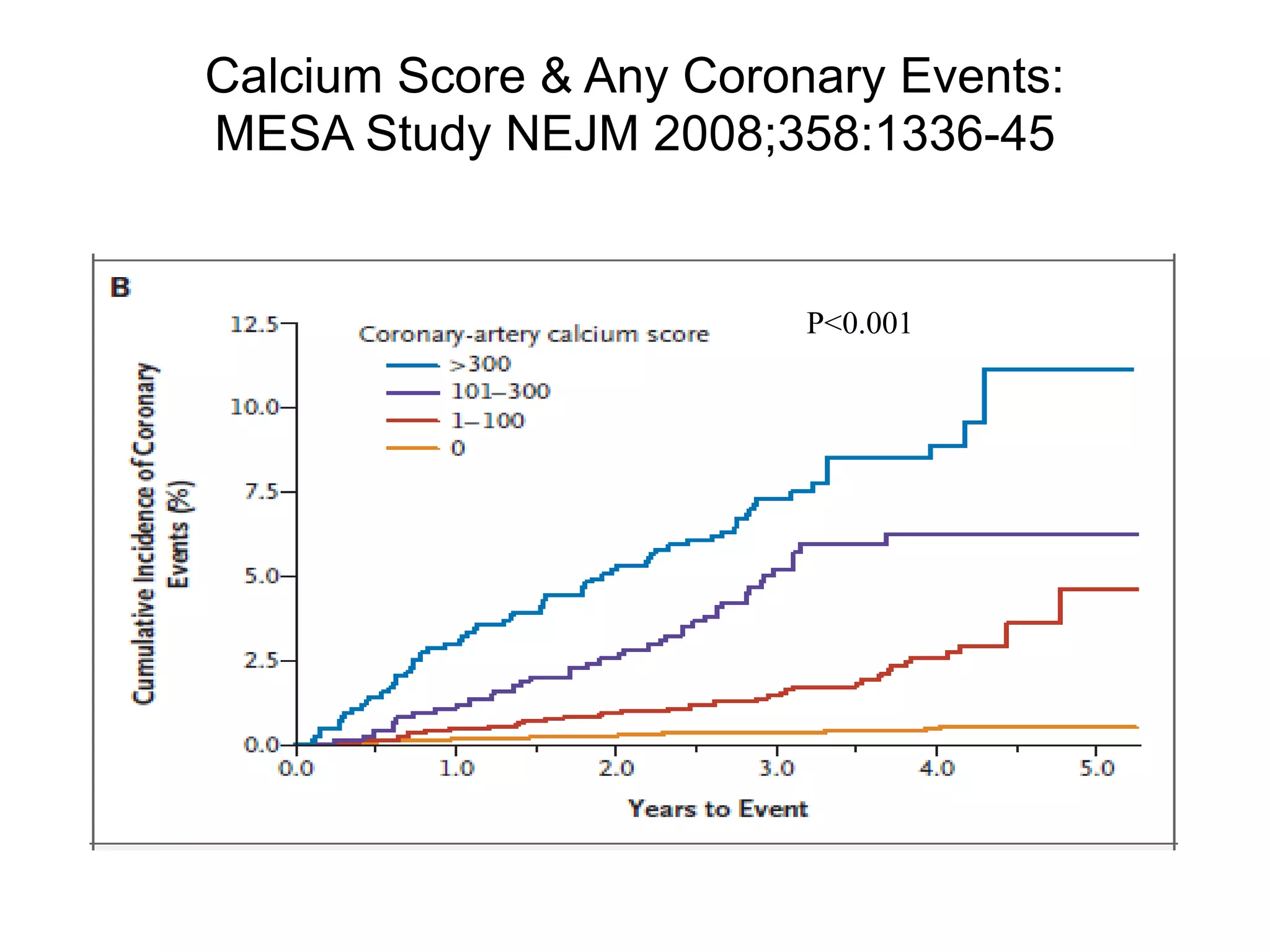
Coronary CT calcium scoring (CAC) is a non-invasive test used to detect calcified plaques in coronary arteries, aiding in the assessment of heart disease risk. Although primarily for asymptomatic patients at intermediate risk, it measures plaque presence rather than the severity of blockage. Benefits include early identification of heart disease risk, while minimal risks are involved due to low radiation exposure.