Downloaded 82 times
![“(Is) Coronary Calcium Scoring: the
Logical Way to Assess CVS Risk?”
“Coronary Calcium Scoring: is challenging
the established [and entrenched?]
epidemiological concepts of CVS risk
assessment ”](https://image.slidesharecdn.com/chriselliscalciumscoringcta-140321054525-phpapp01/85/Chris-ellis-calcium-scoring-cta-2-320.jpg)
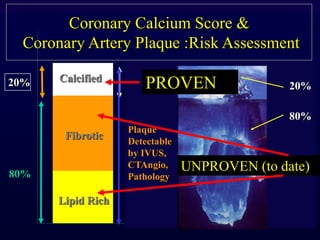
![Calcified Coronary Arteries
• Intuitive for CVS Risk
– Look for disease
– Concept used elsewhere
• Coronary Atherosclerosis &
calcification is the „End
Product‟ of all CVS risk
factors [known or unknown]](https://image.slidesharecdn.com/chriselliscalciumscoringcta-140321054525-phpapp01/85/Chris-ellis-calcium-scoring-cta-8-320.jpg)
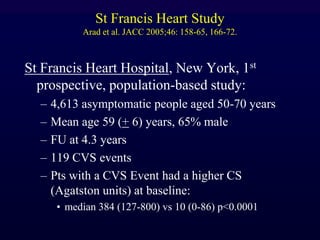
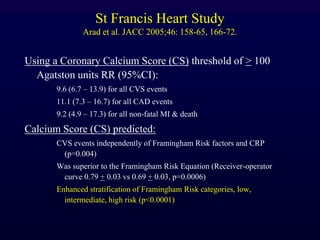
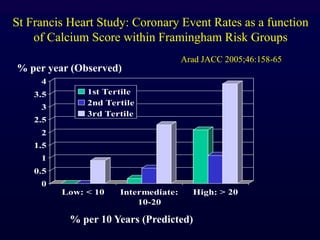
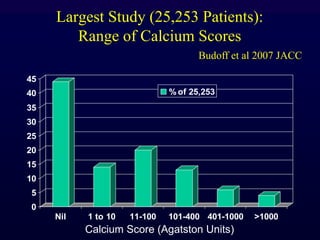
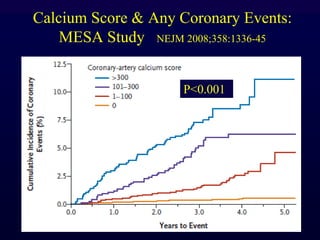
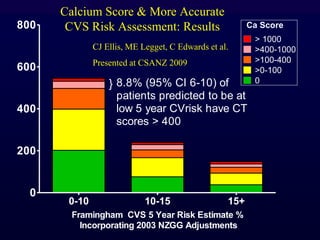
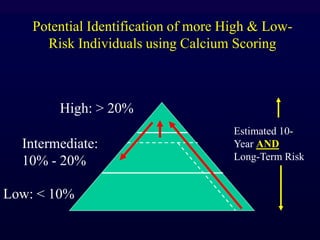

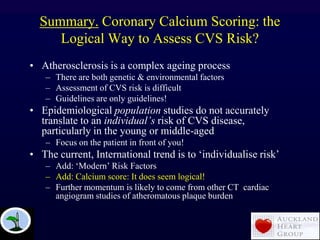

Coronary calcium scoring may be a more logical way to assess cardiovascular risk than established epidemiological models. The document discusses how atherosclerosis is complex and poorly understood, making risk assessment difficult. Studies show calcium scoring independently predicts risk and enhances risk stratification beyond traditional risk factors. Large trials found higher calcium scores strongly associated with future coronary events and mortality. The document argues looking for disease through calcium scoring is more intuitive than using charts or equations without an imaging biomarker of disease. It concludes calcium scoring individualizes risk assessment better than population-based guidelines.













































































