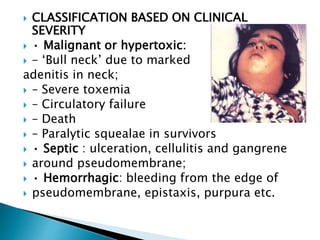
This document summarizes the characteristics and pathogenicity of Corynebacterium diphtheriae, which causes diphtheria. It notes that C. diphtheriae appears as slender, gram-positive rods that can have club-shaped ends and contain metachromatic granules. Infection typically occurs in the upper respiratory tract, where the bacteria's toxin causes a pseudomembrane and systemic effects. Transmission is through droplets or direct contact. Immunization with diphtheria toxoid vaccine provides protection against the disease.