
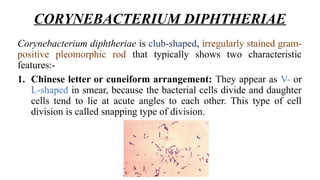
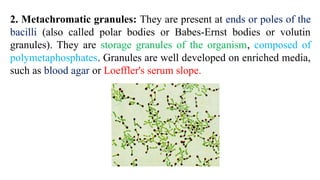

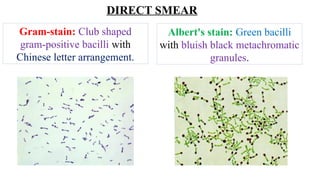

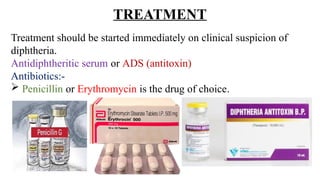


Corynebacterium diphtheriae is a gram-positive, non-motile bacillus responsible for diphtheria, characterized by club-shaped morphology and the presence of metachromatic granules. The virulence factor, diphtheria toxin, mediates the disease's symptoms, which include respiratory issues and systemic complications due to toxin spread, while diagnosis involves culture and biochemical tests. Treatment includes antitoxin and antibiotics, with vaccination using diphtheria toxoid being crucial for prevention.























































































