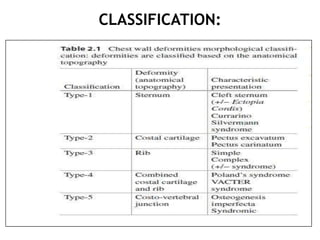
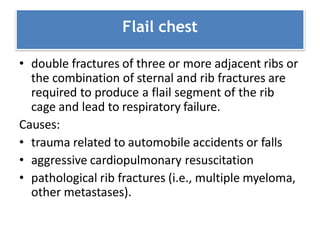
This document discusses various chest wall disorders and deformities including scoliosis, pectus excavatum, flail chest, thoracoplasty, pectus carinatum, and Poland syndrome. Scoliosis is defined as a lateral curvature of the spine and can reduce lung volumes and compliance. Pectus excavatum involves a sunken sternum while pectus carinatum is a protruding sternum. Flail chest involves multiple broken ribs disrupting chest wall motion. Thoracoplasty was previously used to treat tuberculosis by compressing the lung. Surgical repair options are discussed for various conditions.