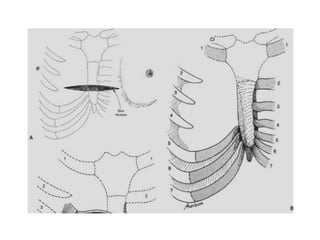
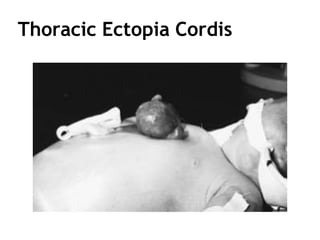
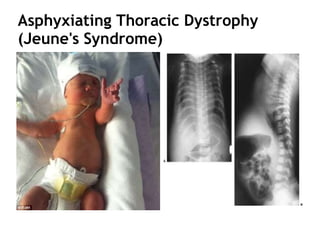
This document summarizes several chest wall disorders and deformities. It describes the classification, symptoms, surgical techniques, and complications for conditions like pectus excavatum, pectus carinatum, Poland's syndrome, cleft sternum, ectopia cordis, and thoracic deformities in diffuse skeletal disorders. Key details are provided on the etiology, incidence, presentation and treatment approaches for each condition.