Download to read offline

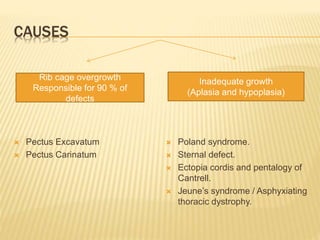
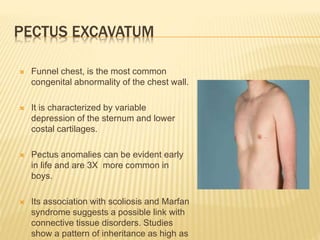
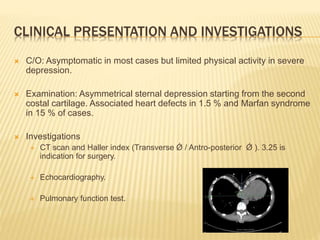
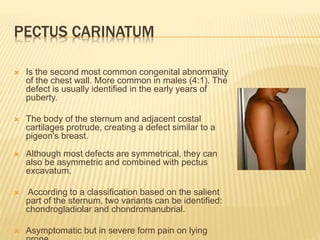


This document discusses various congenital chest wall anomalies including pectus excavatum, pectus carinatum, Poland syndrome, sternal defects, ectopia cordis, Jeune's syndrome, and rib cage overgrowth. It describes the causes, clinical presentations, investigations, and treatment options for each condition. The treatment sections focus on the modified Ravitch procedure, Nuss procedure, osteotomies, muscle flaps, and bracing depending on the specific anomaly.


















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
















