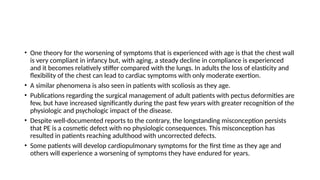
Pectus excavatum is a common congenital chest deformity predominantly affecting males, often leading to significant physiological, psychological, and cosmetic concerns. Symptoms may include dyspnea, fatigue, and palpitations, and the condition can affect cardiac and pulmonary function, which may worsen with age. Surgical correction is indicated for symptomatic patients, with evaluation including imaging and pulmonary function tests, while surgical interventions are generally more successful in older children and adults.







































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
