Downloaded 1,258 times


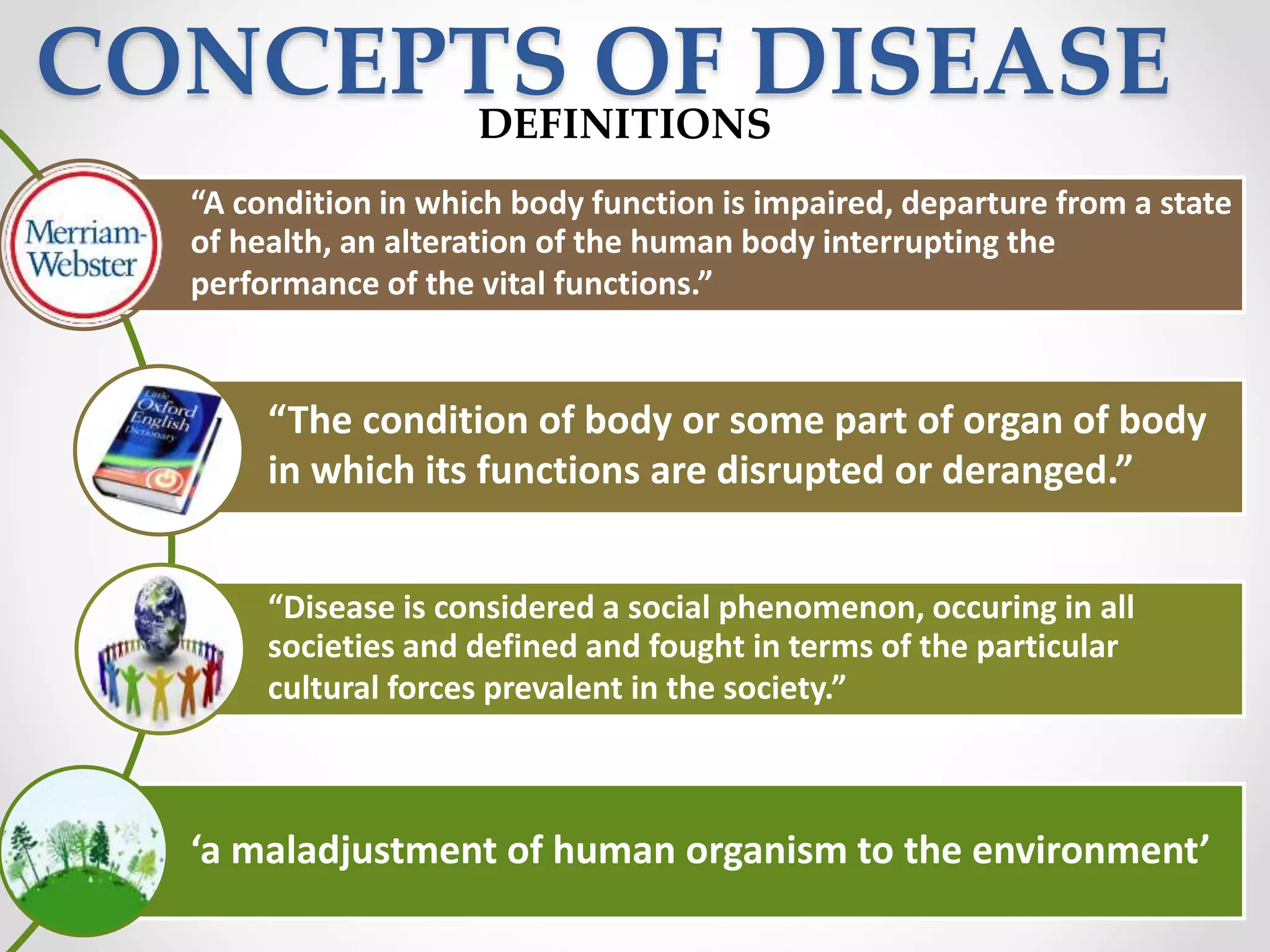

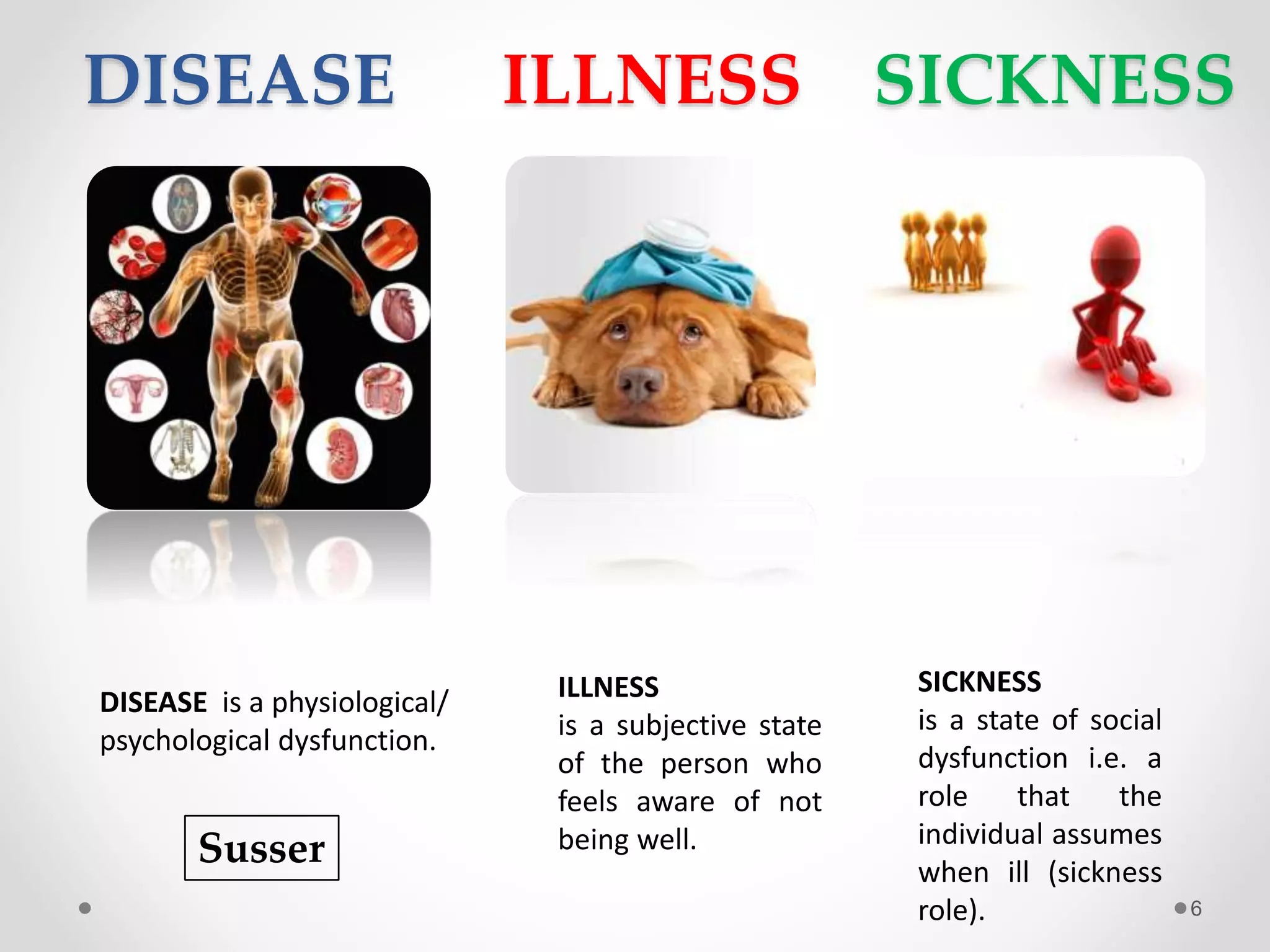


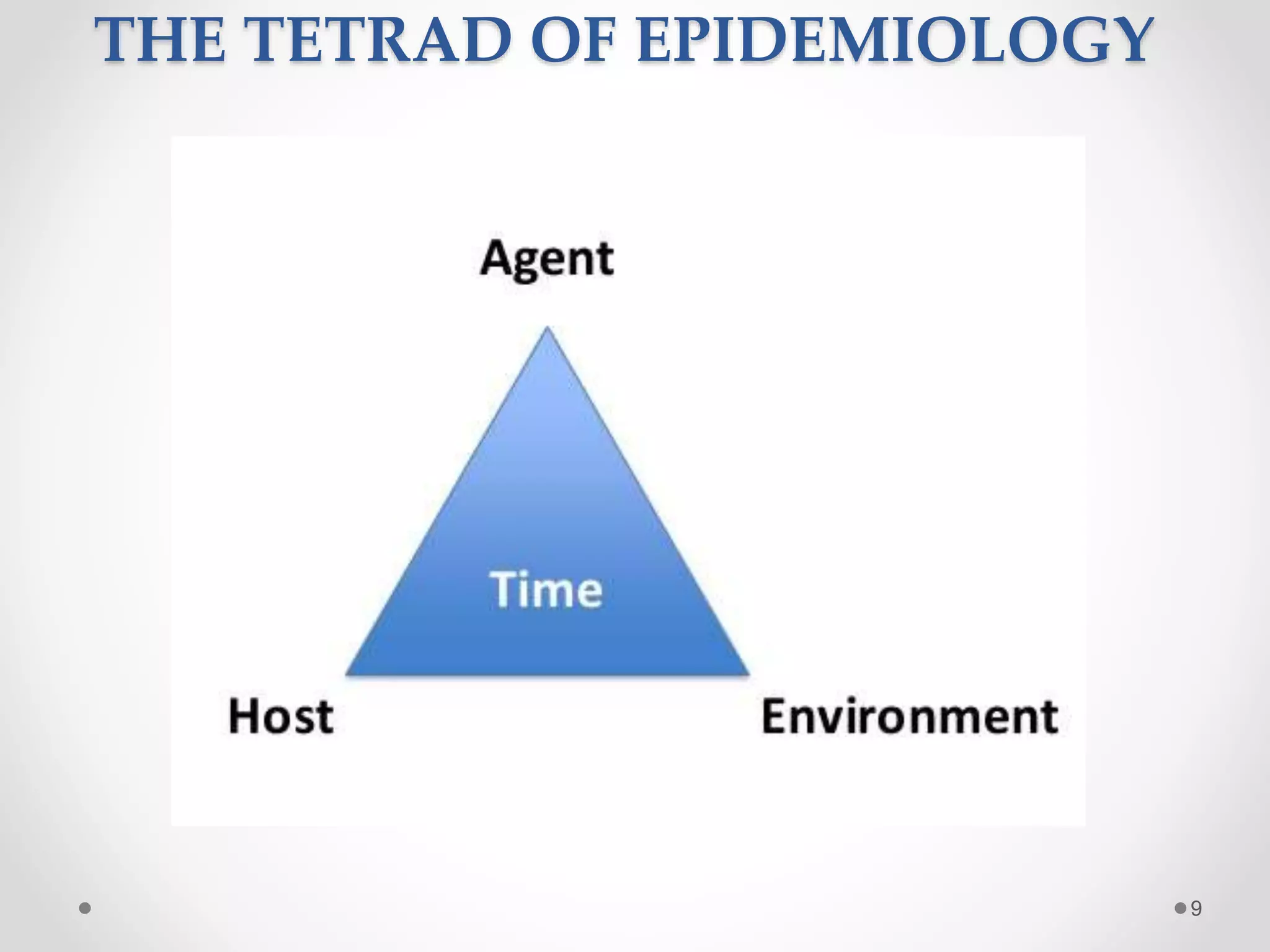
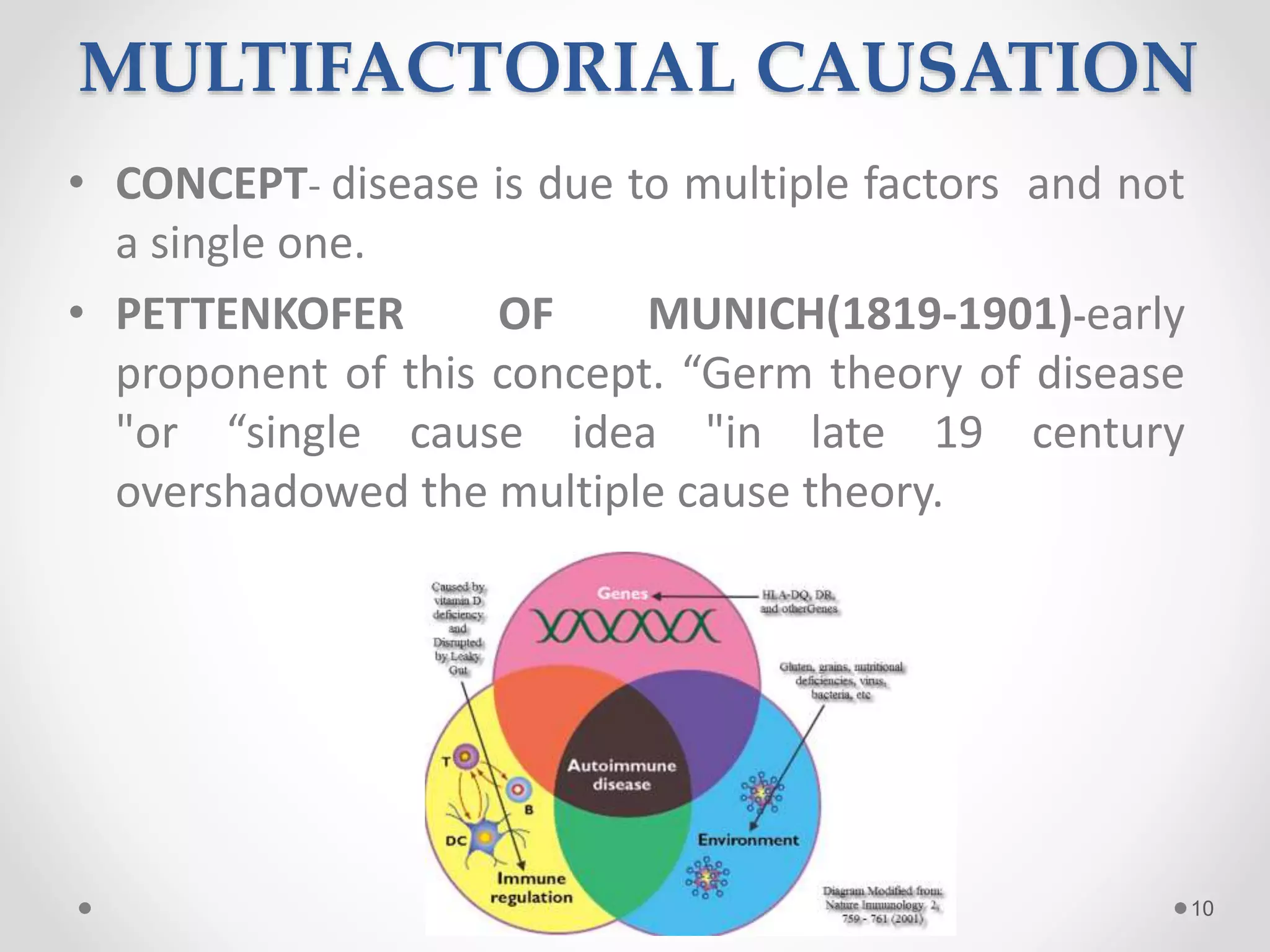

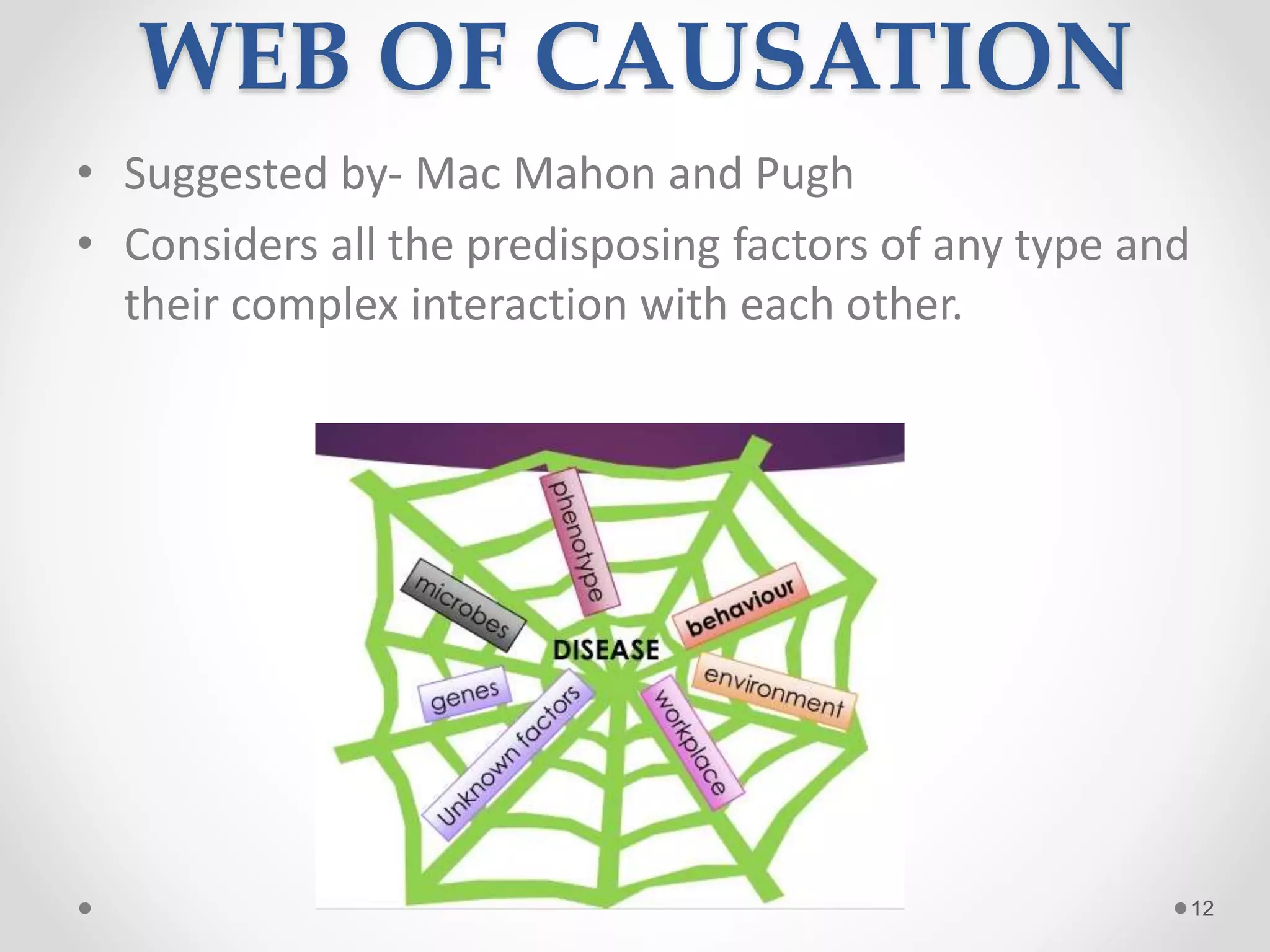


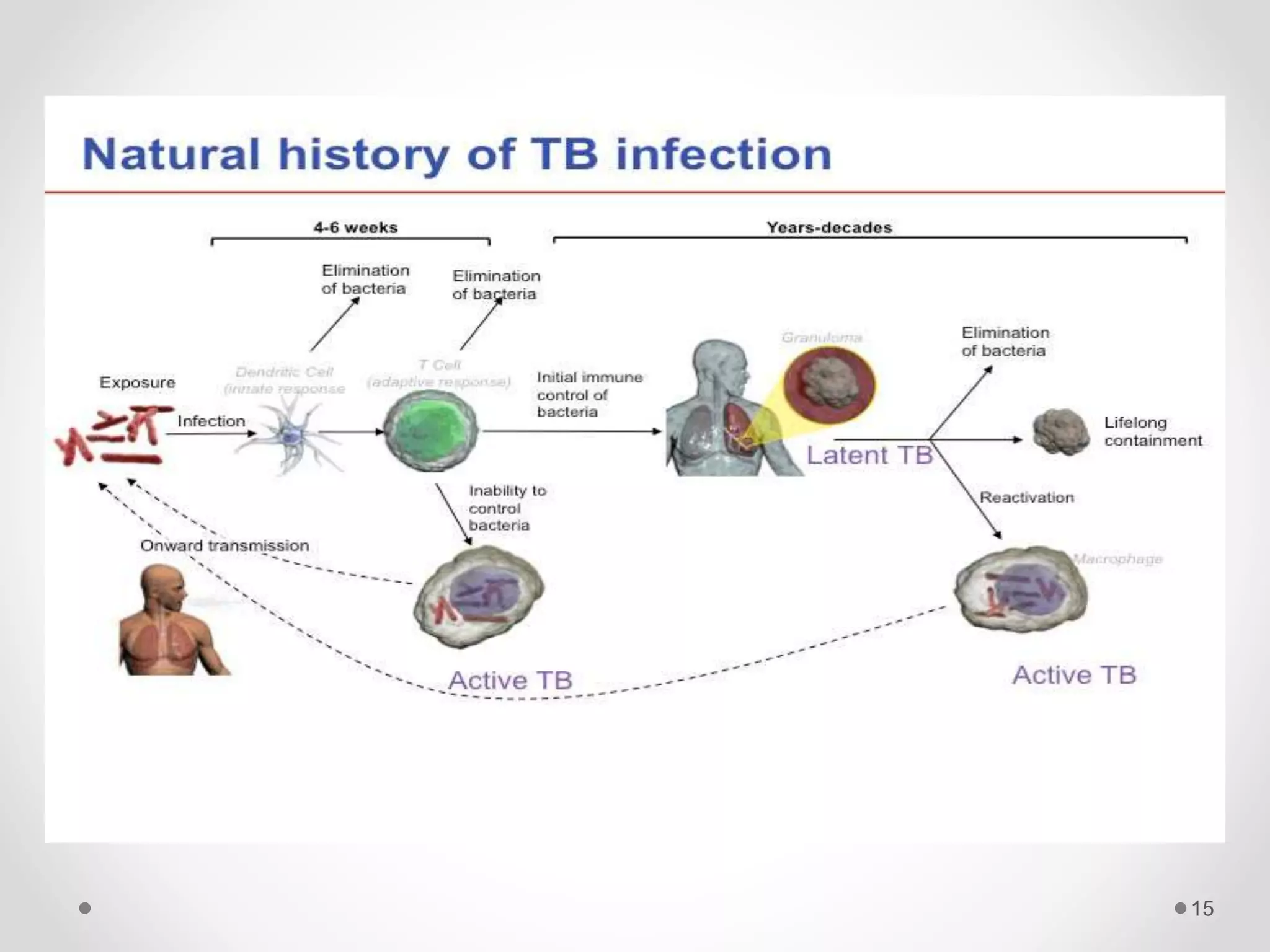


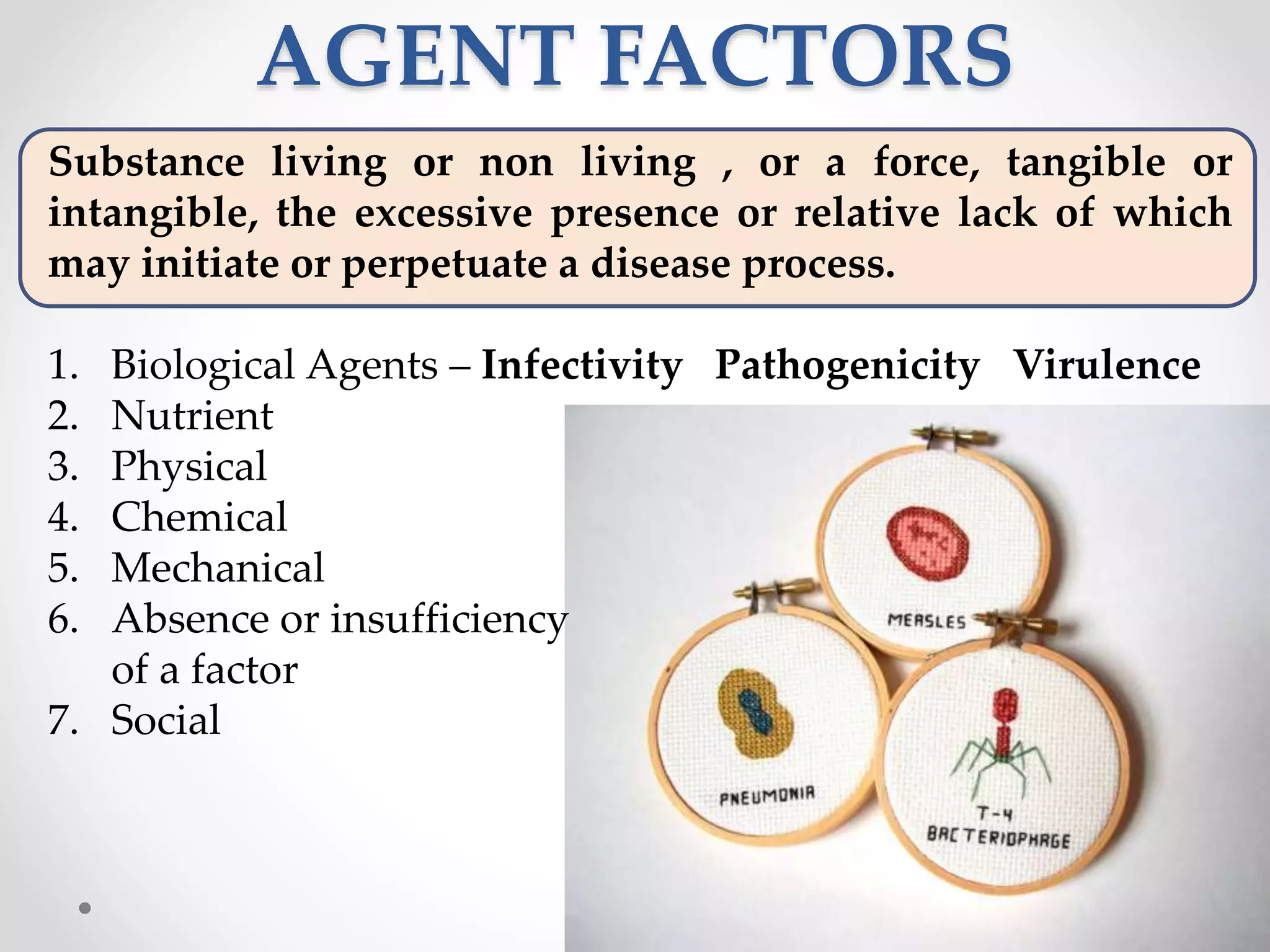
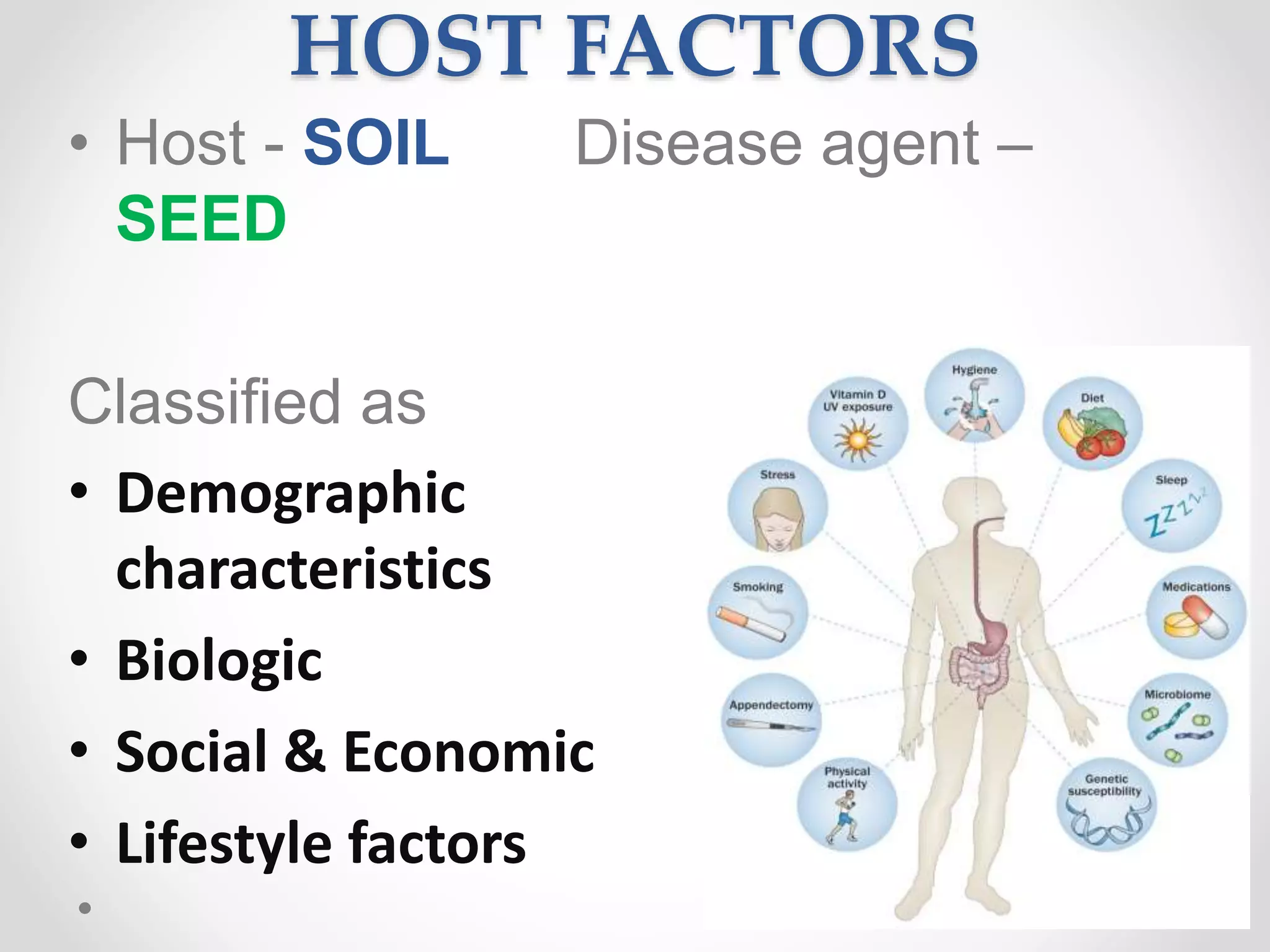


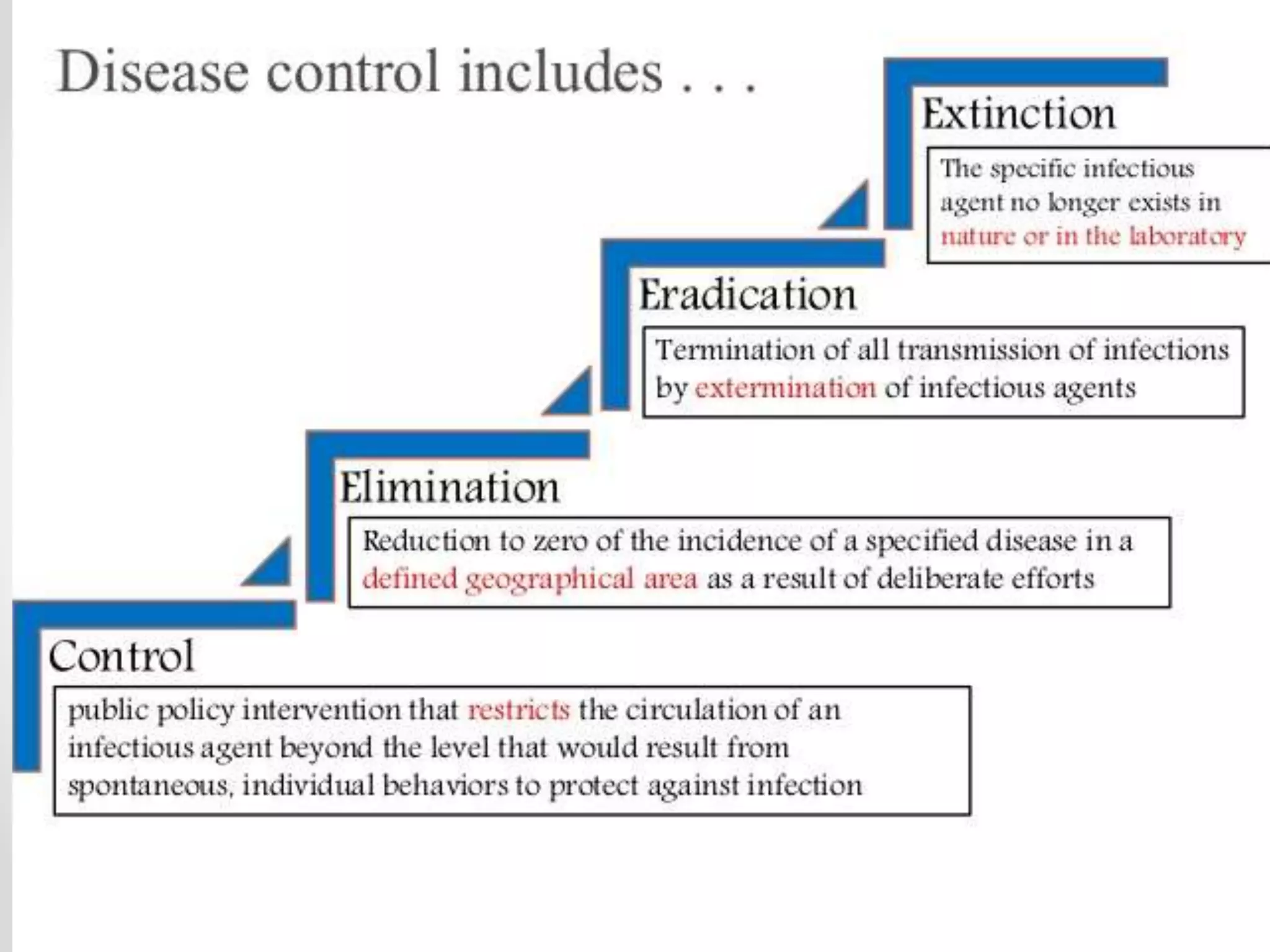












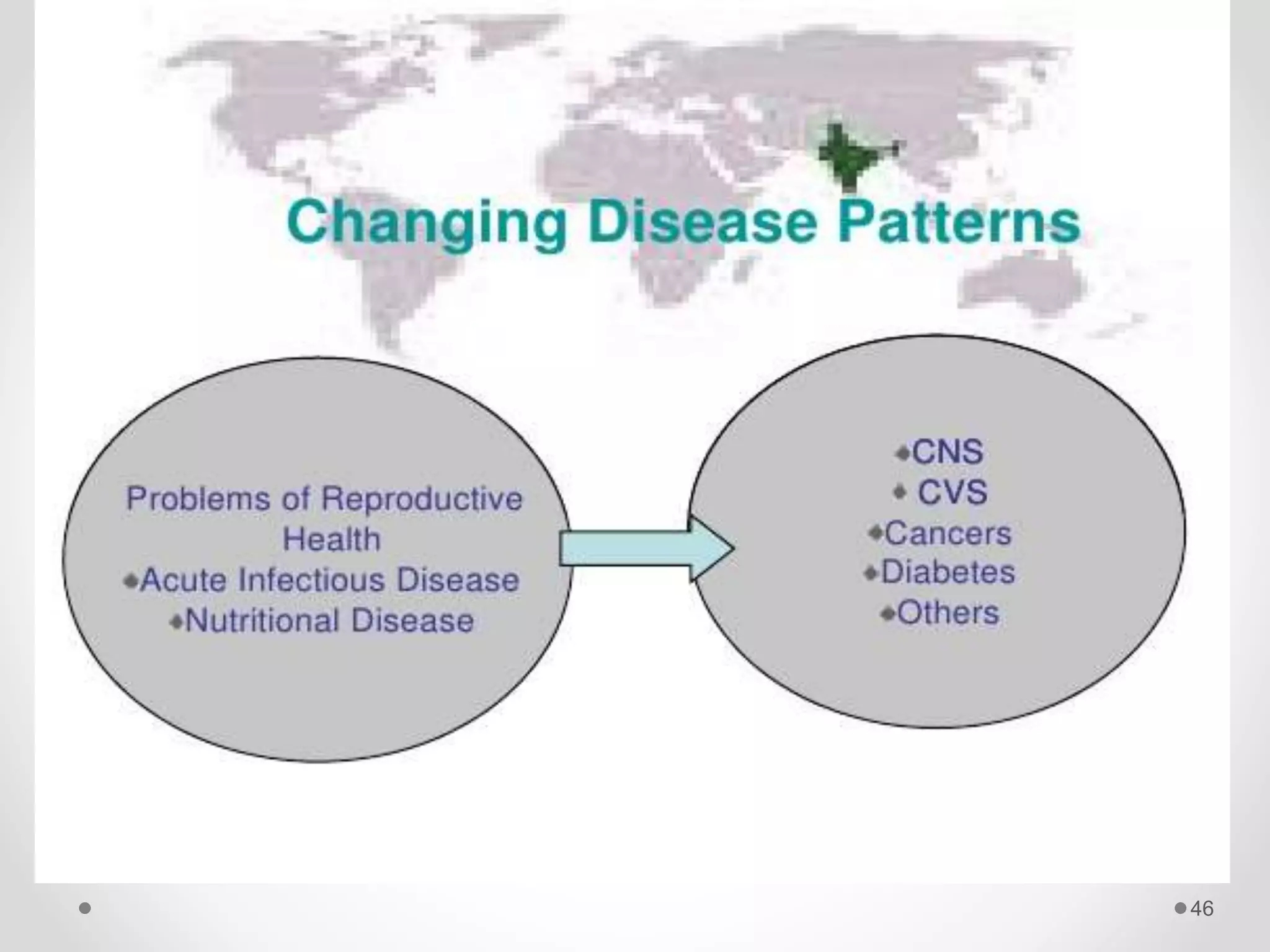







The document discusses concepts of disease including definitions of disease, illness, and sickness, as well as concepts of causation including the epidemiological triad and web of causation. It also covers the natural history of disease, concepts of disease control including disease elimination and eradication, and concepts of disease prevention including the levels of primary, secondary, tertiary, and primordial prevention.























































































