Downloaded 12 times







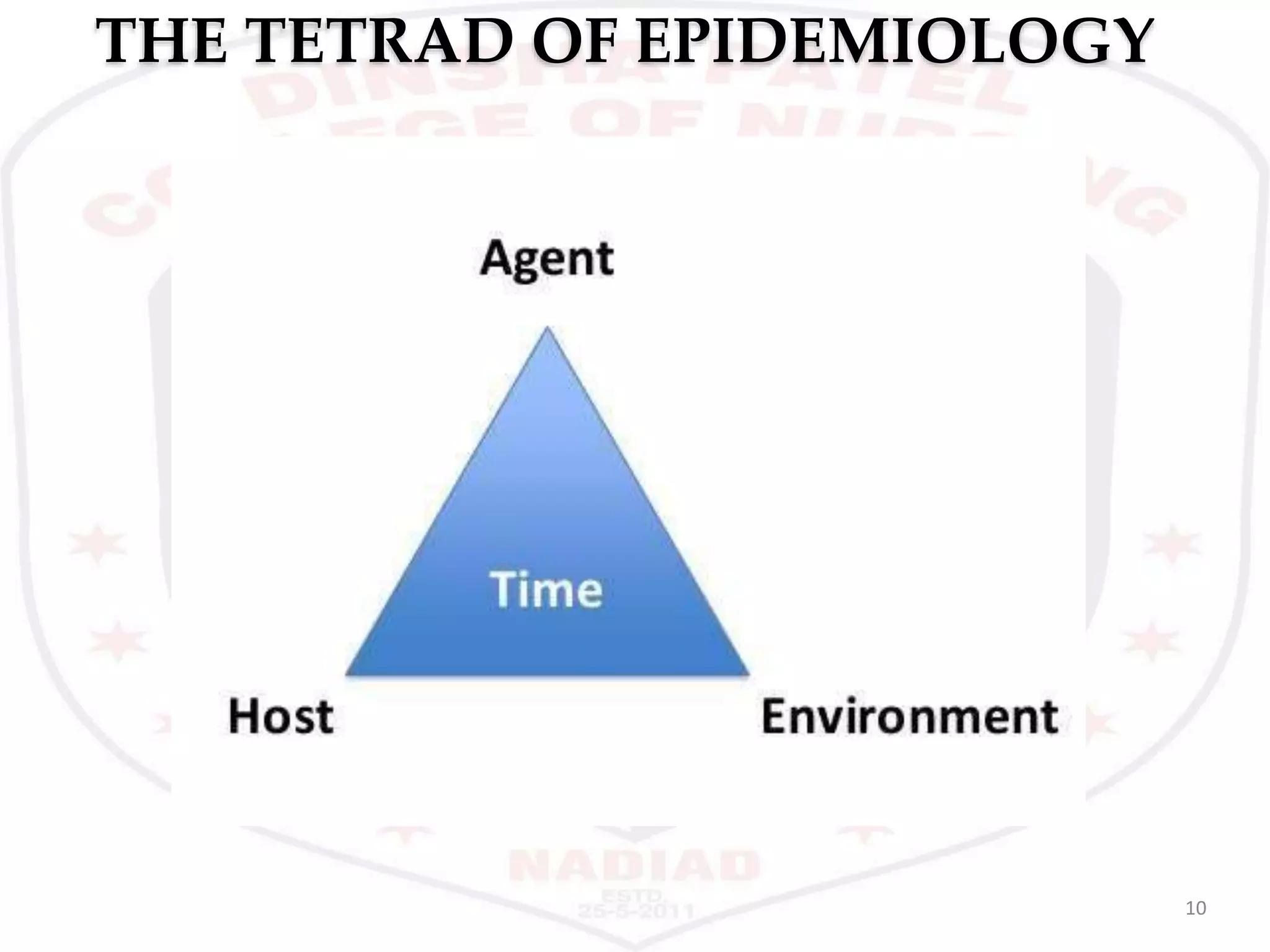




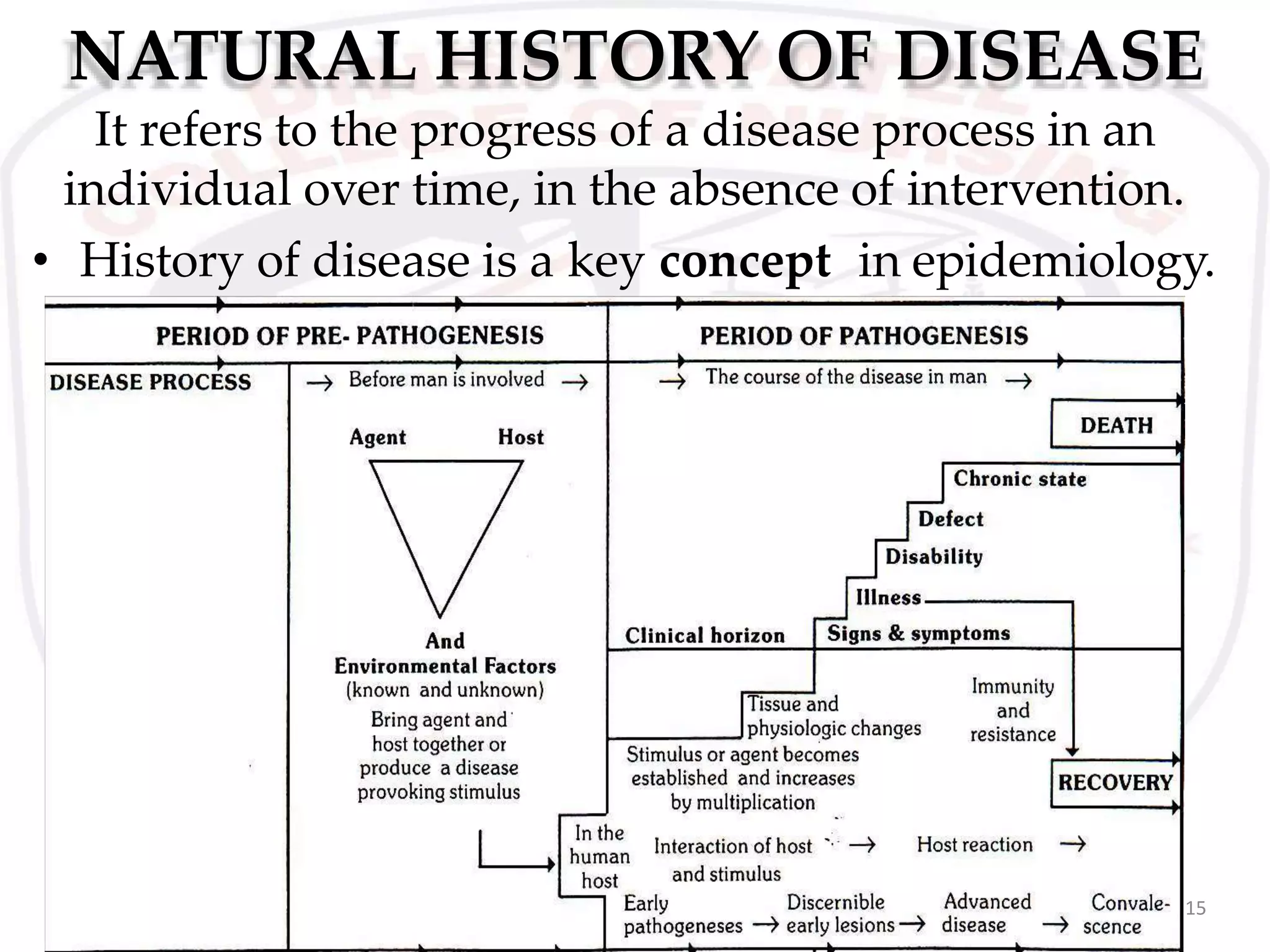

























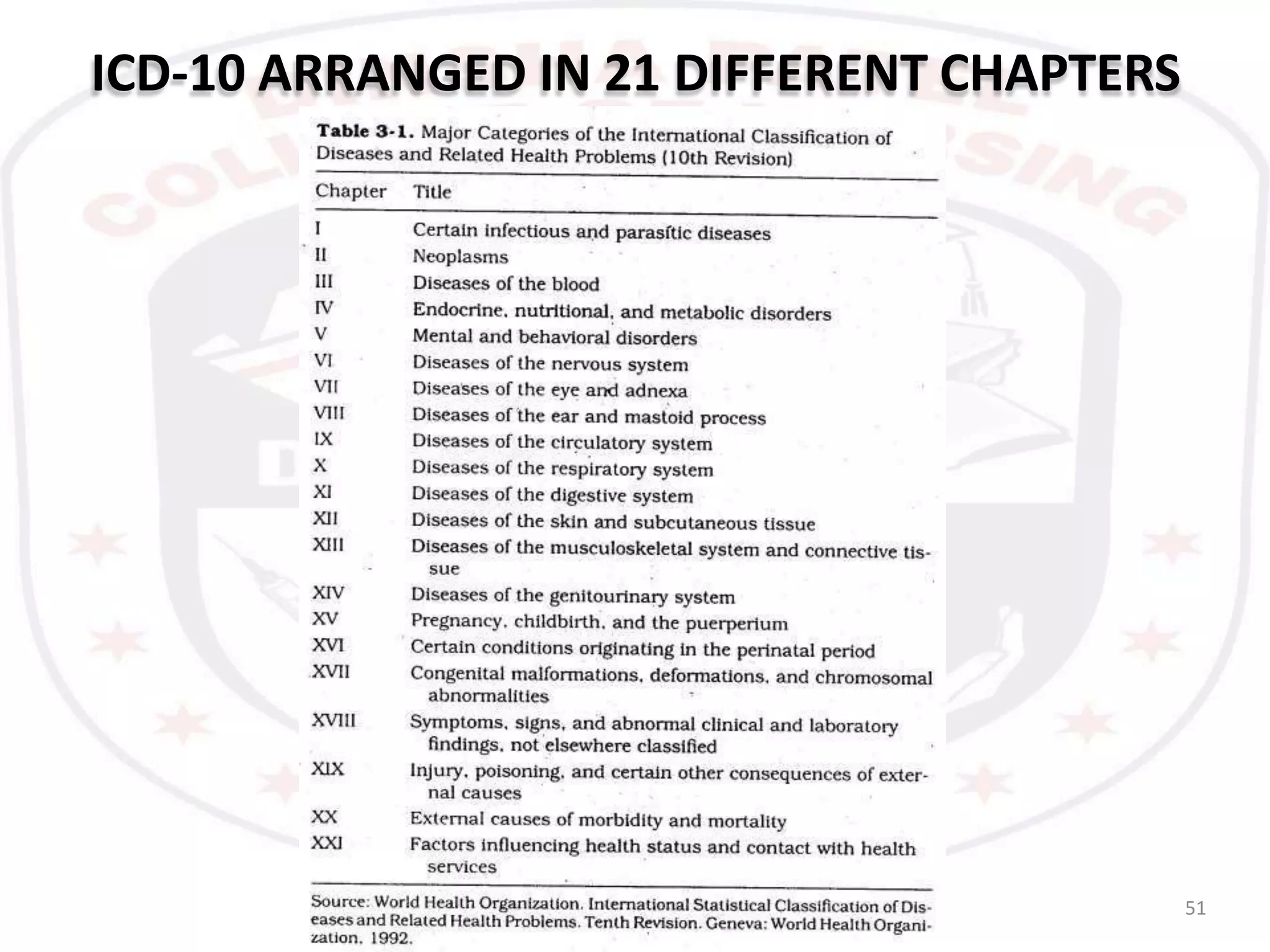




This document provides an overview of key concepts related to disease including definitions of disease, concepts of causation, the natural history of disease, disease classification, and concepts of control and prevention. It discusses definitions of disease from impairments in body function to social phenomena. The concepts of causation are explored from early supernatural and humoral theories to the epidemiological triad and web of causation. The natural history of disease is described through pre-pathogenesis, pathogenesis and spectrum of disease. Levels of prevention including primary, secondary and tertiary are defined. Disease control aims to reduce incidence, duration and effects while concepts like elimination and eradication are explained. The changing patterns of disease and International Classification of Diseases are also summarized















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)






