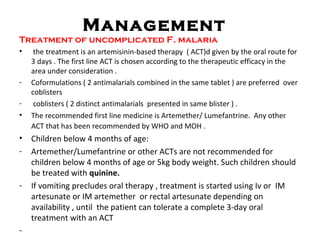
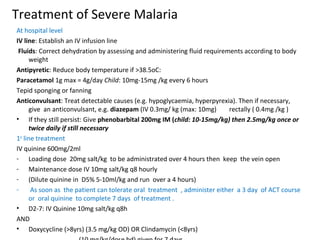
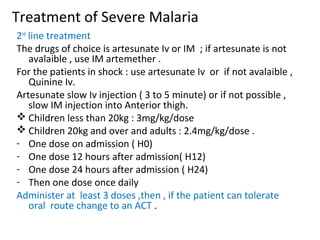
Uncomplicated and severe malaria are described. Uncomplicated malaria is defined as malaria symptoms with a positive test but no severe features, while severe malaria almost always involves P. falciparum and can be life-threatening. Treatment of uncomplicated malaria involves ACT like artemether-lumefantrine for 3 days. Severe malaria requires hospitalization and IV treatment with quinine or artesunate, along with managing complications and symptoms. Studies in Somalia found unacceptably high failure rates for artemether-sulfadoxine/pyrimethamine, indicating a need to replace it with a more effective ACT.








































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

















