Downloaded 23 times











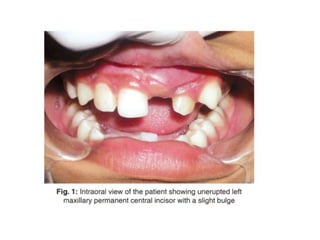
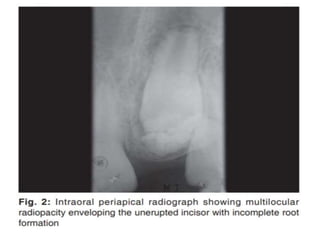





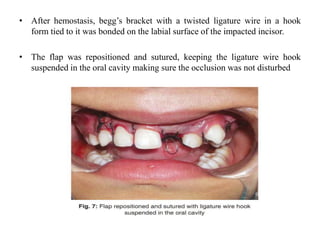









This document presents a case report of a complex odontome obstructing the eruption of a maxillary central incisor in a 12-year old female patient. Radiographs and surgical removal revealed several irregular calcified masses composed of dental tissues. Histopathological examination confirmed the diagnosis of a complex odontome. The odontome was removed and the impacted tooth was left to monitor eruption. Early diagnosis and removal of odontomes can allow for normal eruption of impacted permanent teeth.









































































