Downloaded 72 times


























![REFERENCES
● Key Findings [Internet]. Available from:
https://npcbvi.mohfw.gov.in/writeReadData/mainlinkFile/File341.pdf.
● National programme for control of blindness and vision 2020 [Internet]. www.slideshare.net. 2020 [cited
2023 Dec 25]. Available from: https://www.slideshare.net/ObaidurRehman74/national-programme-for-
control-of-blindness-and-vision-2020
● National Programme For Control of Blindness [Internet]. www.slideshare.net. 2021 [cited 2023 Dec 25].
Available from: https://www.slideshare.net/ShubhangiHedau/national-programme-for-control-of-
blindness-244371540.
● National programme for control of blindness [Internet]. www.slideshare.net. 2017 [cited 2023 Dec 25].
Available from: https://www.slideshare.net/DocSantoshSoren/national-programme-for-control-of-
blindness-80650317.
● · NPCB.pptx [Internet]. www.slideshare.net. 2022 [cited 2023 Dec 25]. Available from:
https://www.slideshare.net/AlmiAlmi1/npcbpptx.
● · Vision 2020 [Internet]. www.slideshare.net. 2015 [cited 2023 Dec 25]. Available from:
https://www.slideshare.net/sssihmspg/vision-2020-54296753.](https://image.slidesharecdn.com/nationalblindnessprogramme-240112222508-ea77d3da/85/national-blindness-control-programme-pptx-36-320.jpg)
![● Krishna N. NATIONAL PROGRAMME FOR CONTROL OF BLINDNESS(NPCB) [Internet].
[cited 2023 Dec 25]. Available from:
https://www.kimsmedicalcollege.org/cme/NAVYA%20KRISHNA-
NATIONAL%20PROGRAMME%20FOR%20CONTROL%20OF%20BLINDNESS.pdf.
● Avachat, Shubhada & Kamble, Suchit & Phalke, Deepak & Bangal, Surekha & Zambare,
Mrinal. (2013). Magnitude causes and management of avoidable blindness: A cross-
sectional study in Pravara Rural Hospital of Rural Medical College, Maharashtra, India.
South East Asia Journal of Public Health.
● JCDR - A Study to Evaluate the Causes of Delayed Presentation for Cataract Surgery at a
Tertiary Eye Centre, Odisha, India [Internet]. www.jcdr.net. [cited 2023 Dec 25]. Available
from: https://www.jcdr.net/article_abstract.asp?issn=0973-
709x&year=2022&volume=16&issue=1&page=NC01&issn=0973-709x&id=15867](https://image.slidesharecdn.com/nationalblindnessprogramme-240112222508-ea77d3da/85/national-blindness-control-programme-pptx-37-320.jpg)


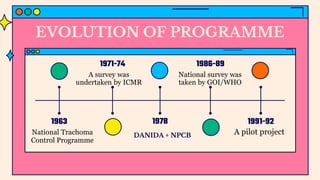
The National Programme for Control of Blindness (NPCB) was initiated in India in 1976 with the goal of reducing blindness prevalence to 0.3% by 2020, focusing on causes such as cataracts and conducting activities like cataract surgeries and community awareness programs. Recent updates include a mission mode campaign, expansion of coverage to various visual impairments, and collaboration with NGOs to enhance eye care services. Studies reveal significant factors affecting timely access to cataract surgery, including financial constraints, fears, and social influences among disadvantaged populations.























































































