
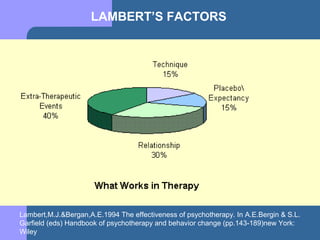


This document outlines the common factors approach to counseling and psychotherapy. It discusses several common factors models, including those proposed by Fisher and Lambert. Fisher identified four common factors: the therapeutic relationship, shared worldview, client expectations, and ritual or intervention. Lambert identified five common factors: the therapeutic relationship, client variables, technique/model, placebo, and expectancy. The document also discusses the importance of the working alliance and addressing alliance ruptures when they occur. It emphasizes applying common factors through a culturally-informed lens and considering factors like a counselor's expertise, credibility, and use of cultural rituals or interventions.































































































