Downloaded 122 times
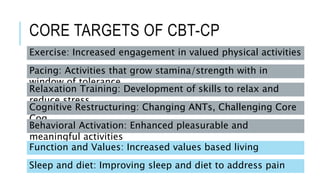
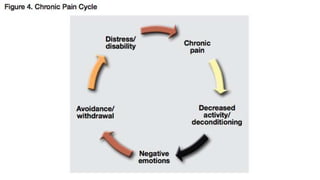
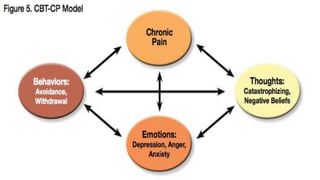
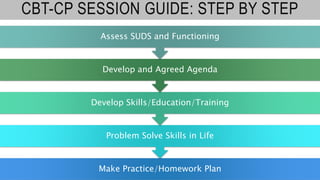
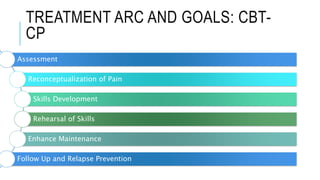
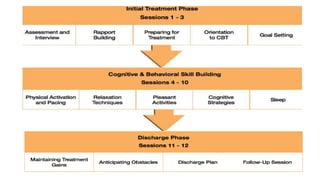

This document provides an overview of cognitive behavioral therapy for chronic pain (CBT-CP). It discusses the core targets of CBT-CP which include exercise, pacing, relaxation training, cognitive restructuring, behavioral activation, function and values, and sleep and diet. It also covers psychological factors like cognitions, catastrophizing, suffering vs. pain, hurt vs. harm, negative affect, answer-seeking, and pain self-efficacy. Behavioral factors like passive coping, resting/inactivity, exercise, and over activity are examined. The document provides guidance on pacing and relaxation training. It also touches on social factors patients with chronic pain may face and provides a case conceptualization example.


























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












