Downloaded 43 times

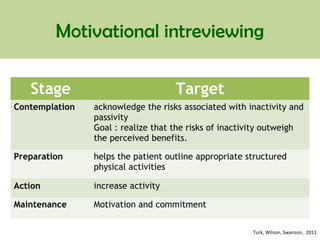
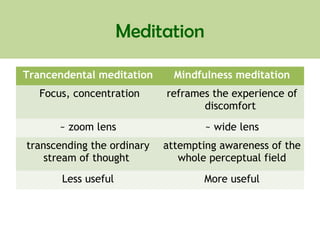

This document discusses various psychological approaches for managing chronic pain, including cognitive behavioral therapy (CBT), relaxation techniques, biofeedback, hypnosis, and motivational interviewing. It notes that CBT is the most common approach and aims to change maladaptive thoughts and behaviors. Relaxation methods like meditation, guided imagery, and biofeedback teach patients to control physiological processes linked to pain. The evidence for different approaches is reviewed, with hypnosis found most useful for acute rather than chronic pain. A conclusion drawn is that multidisciplinary programs combining several treatment components from a collaborative team are most effective for improving chronic pain outcomes.























































































