Downloaded 25 times
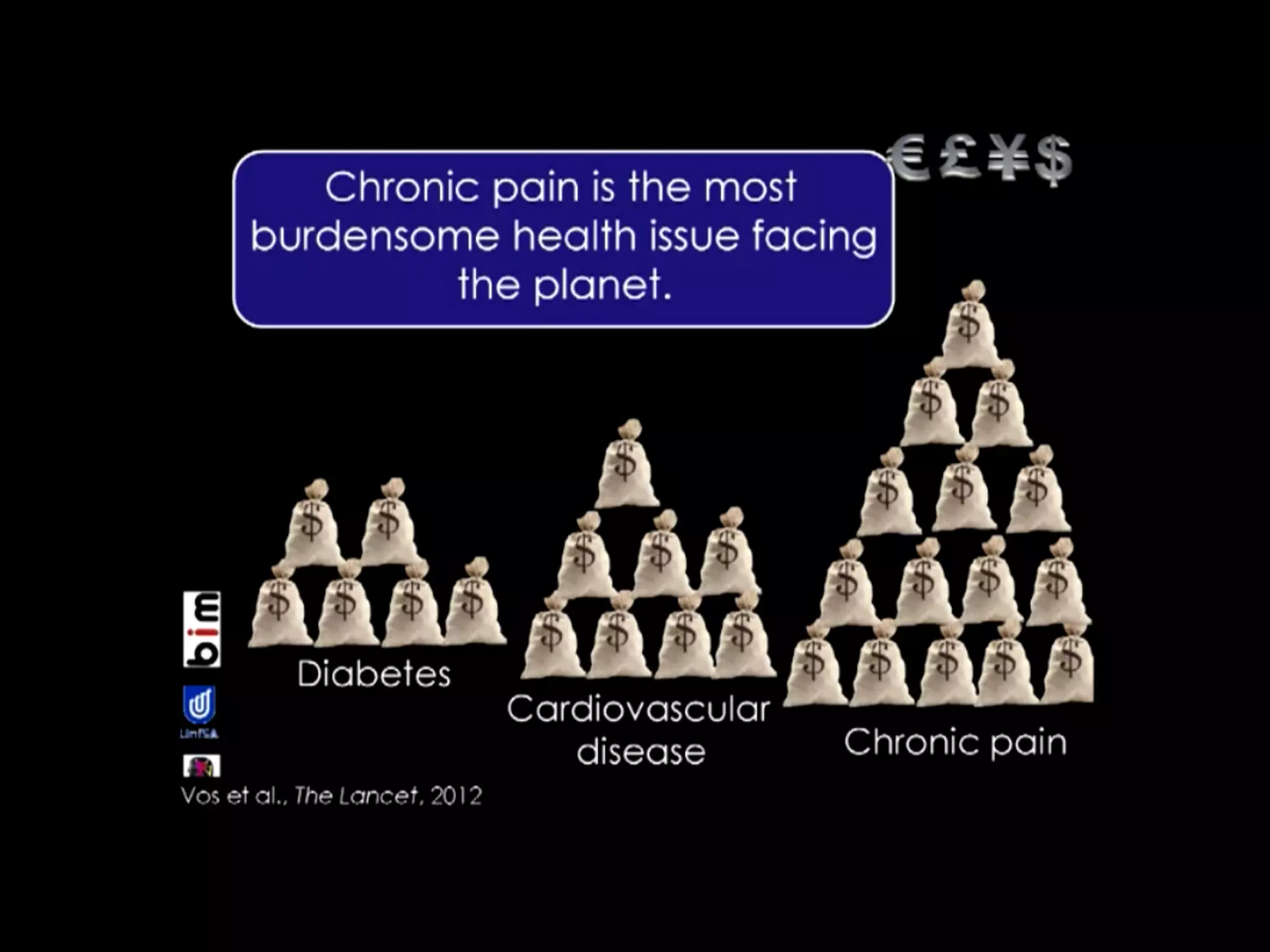
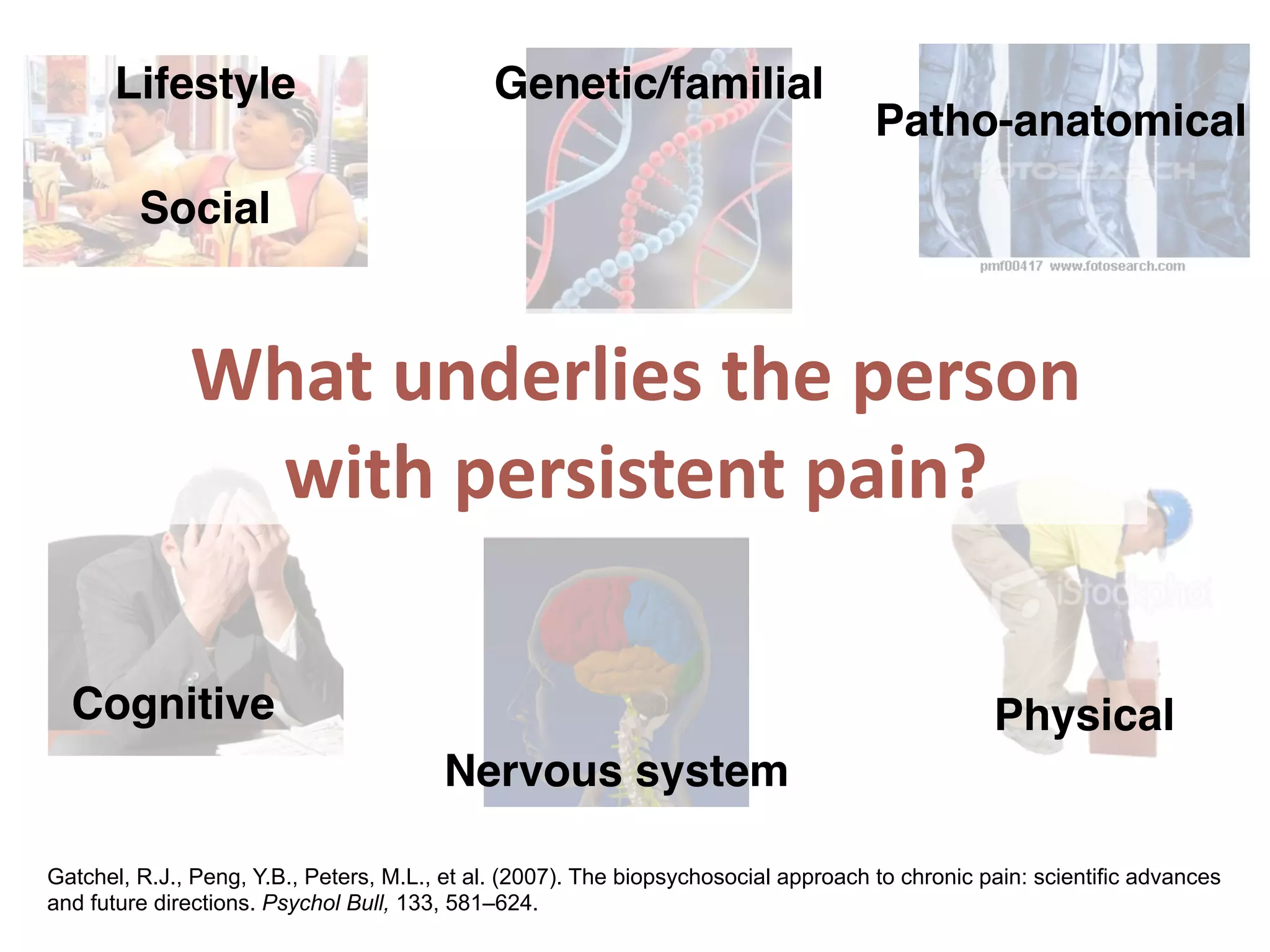
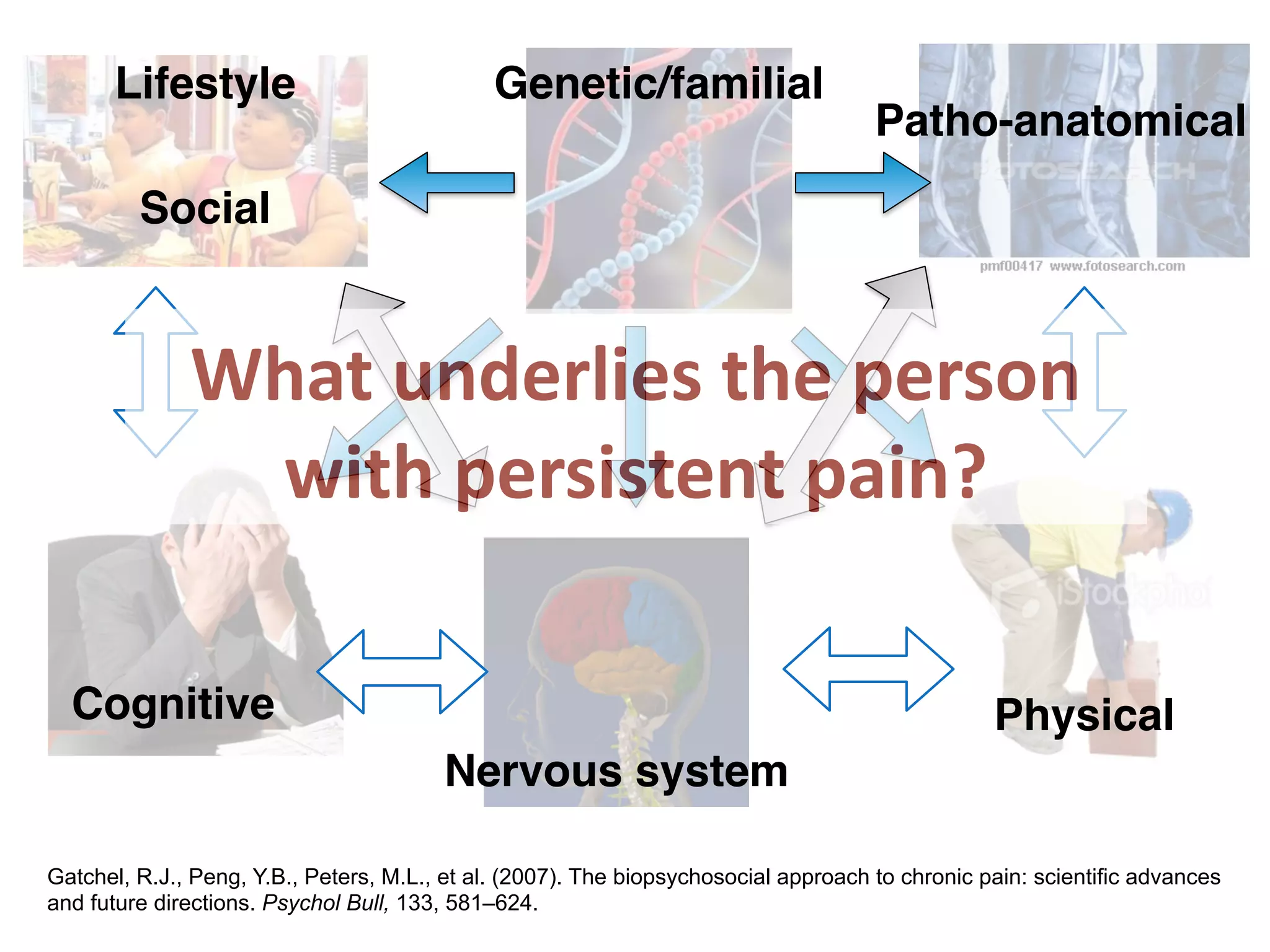
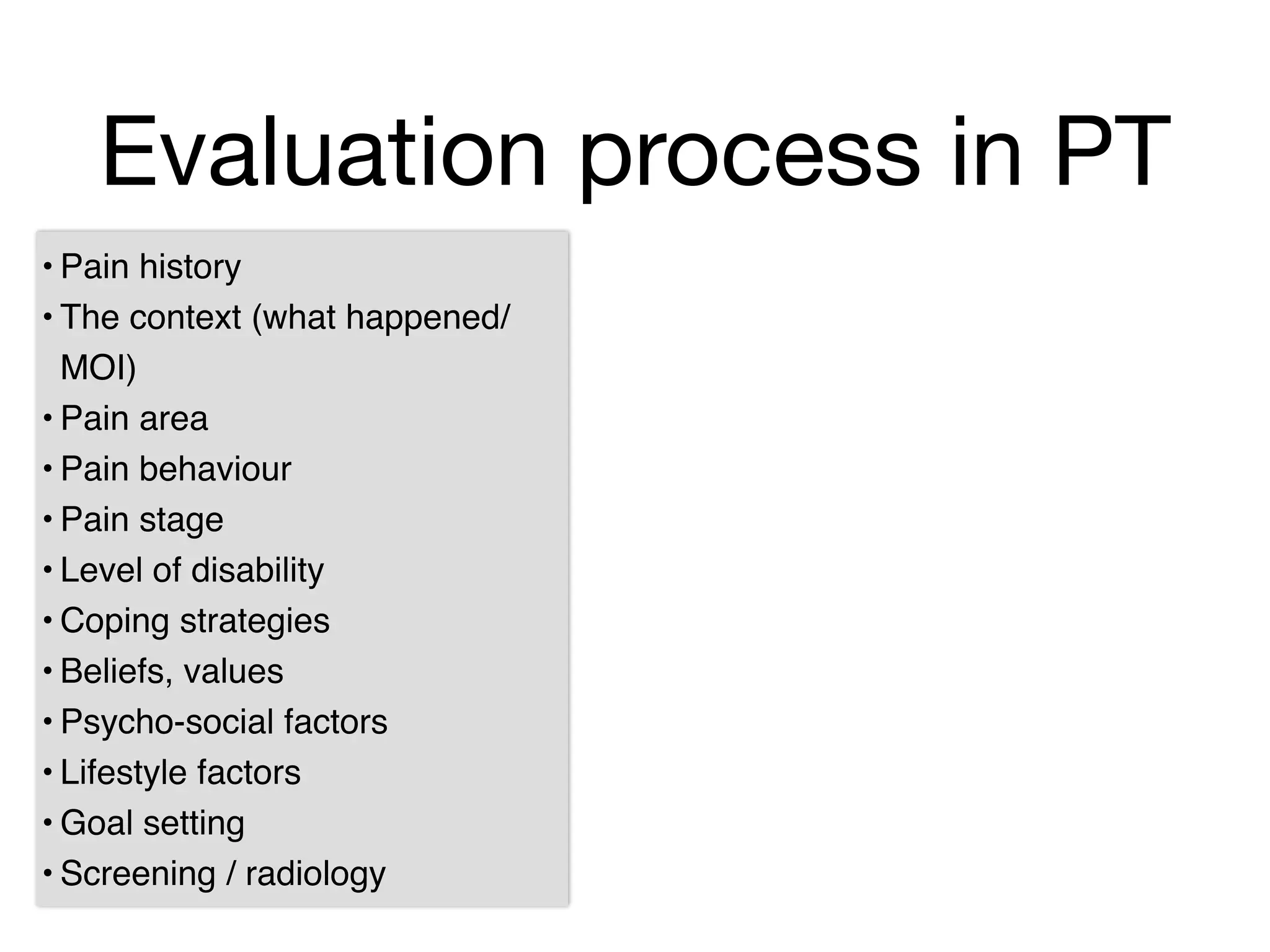
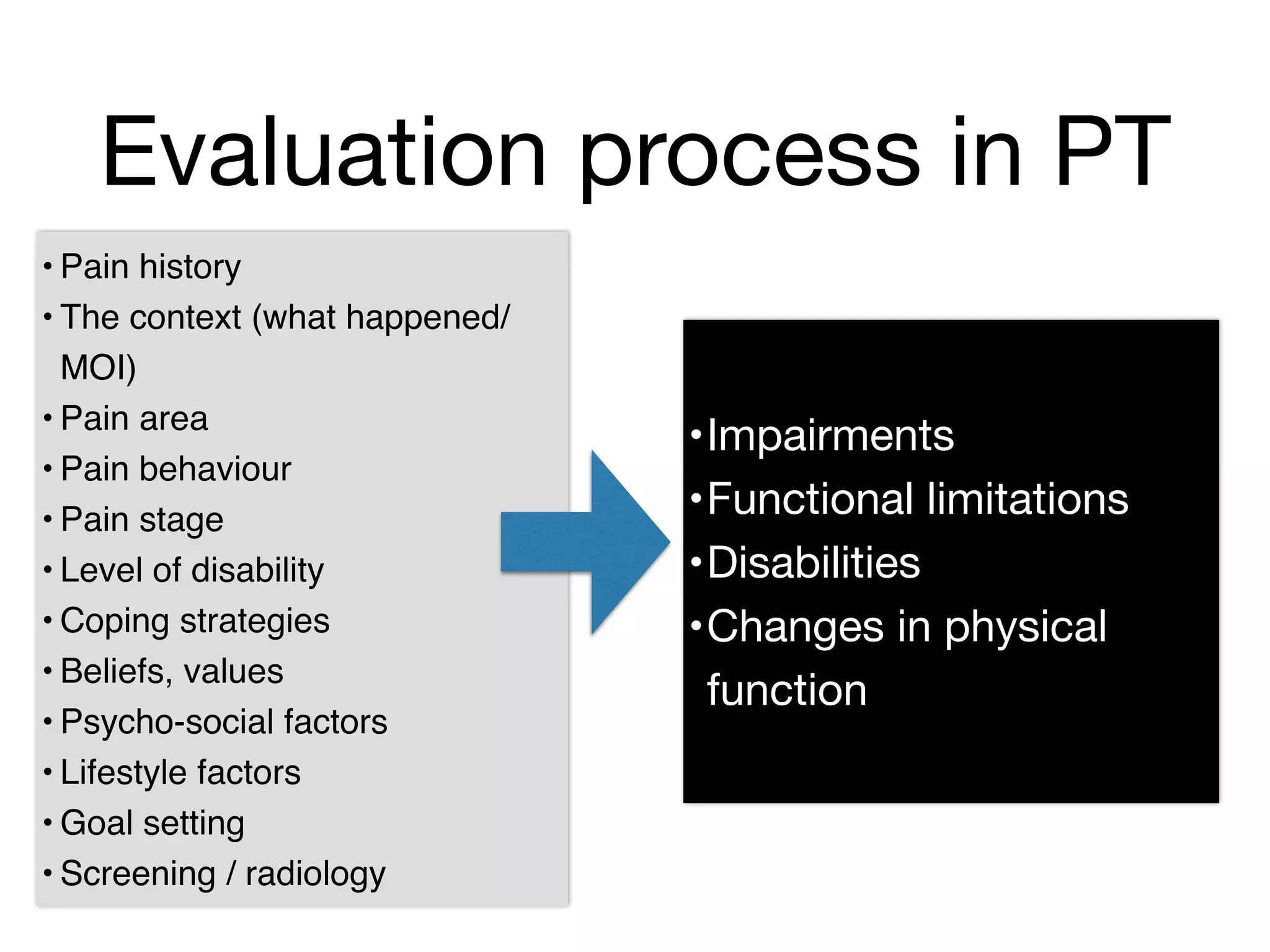
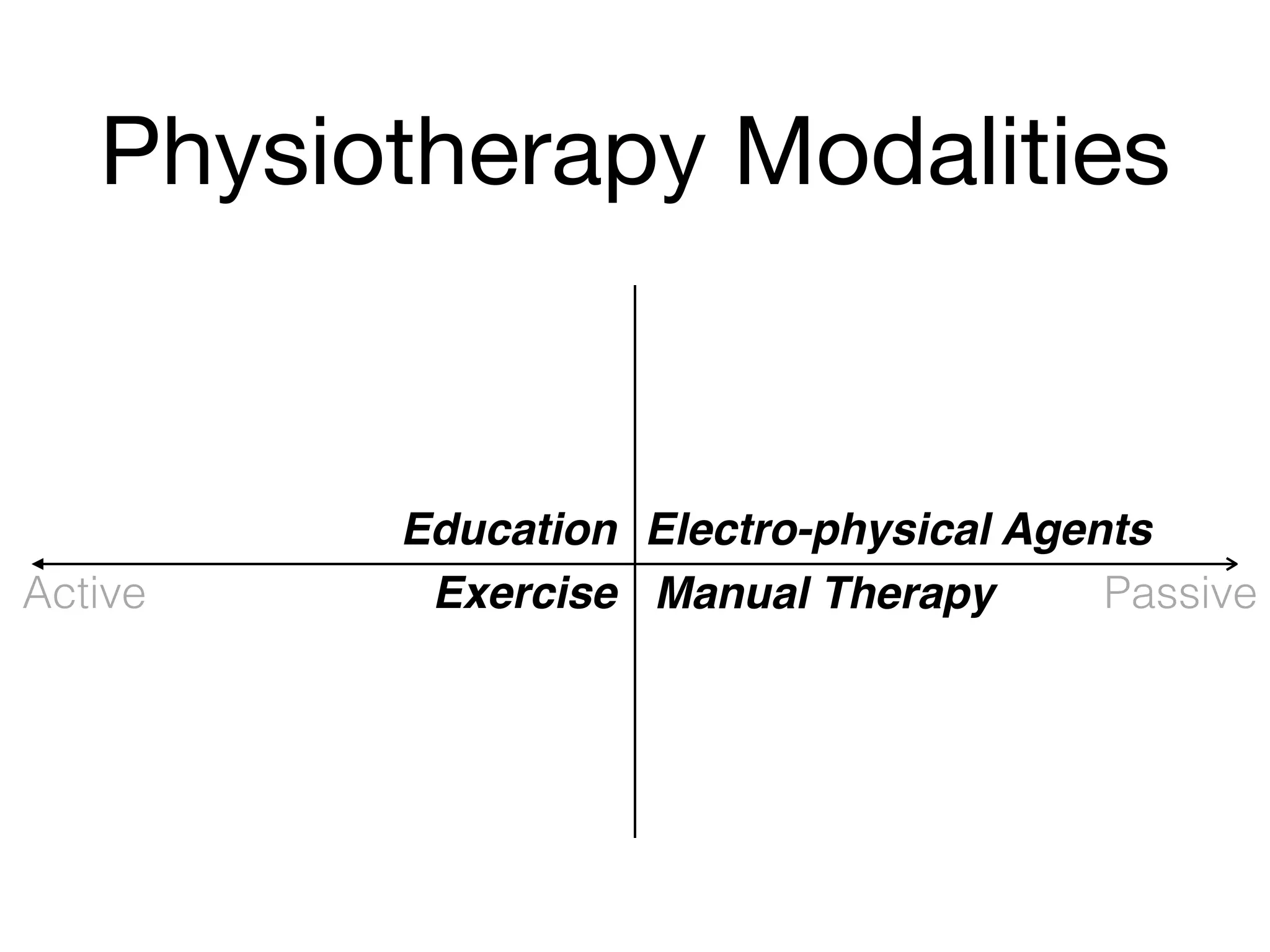
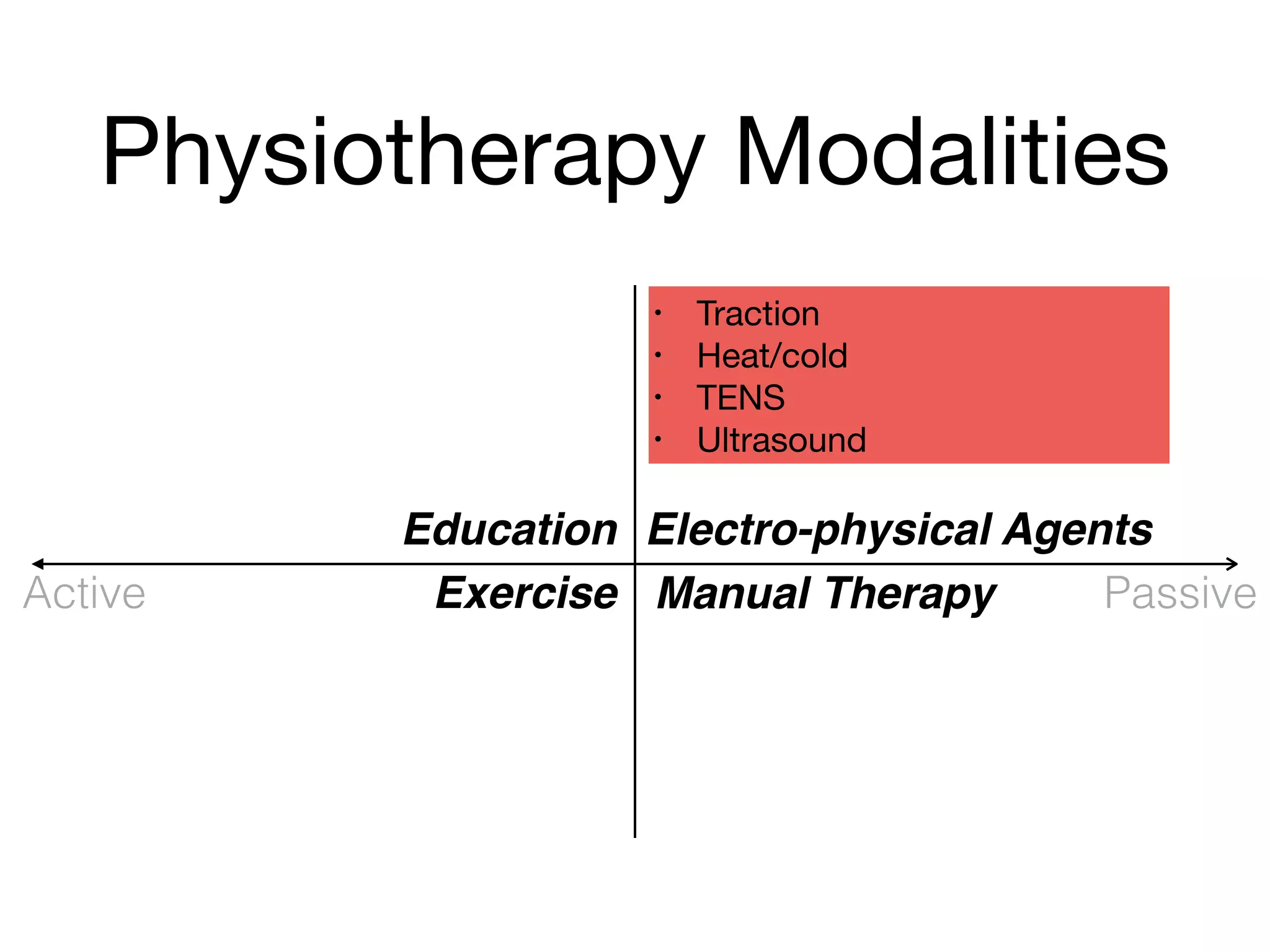
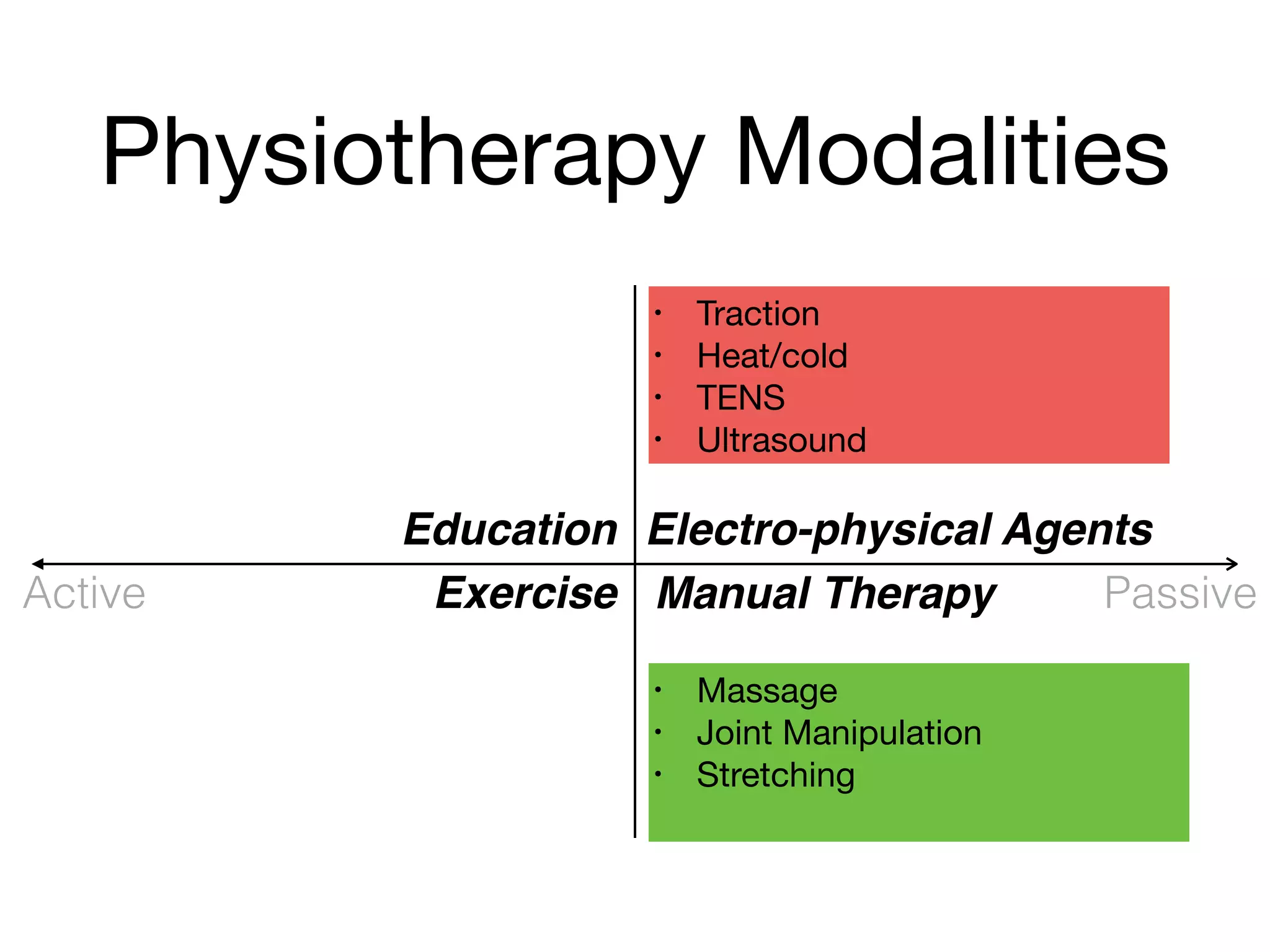
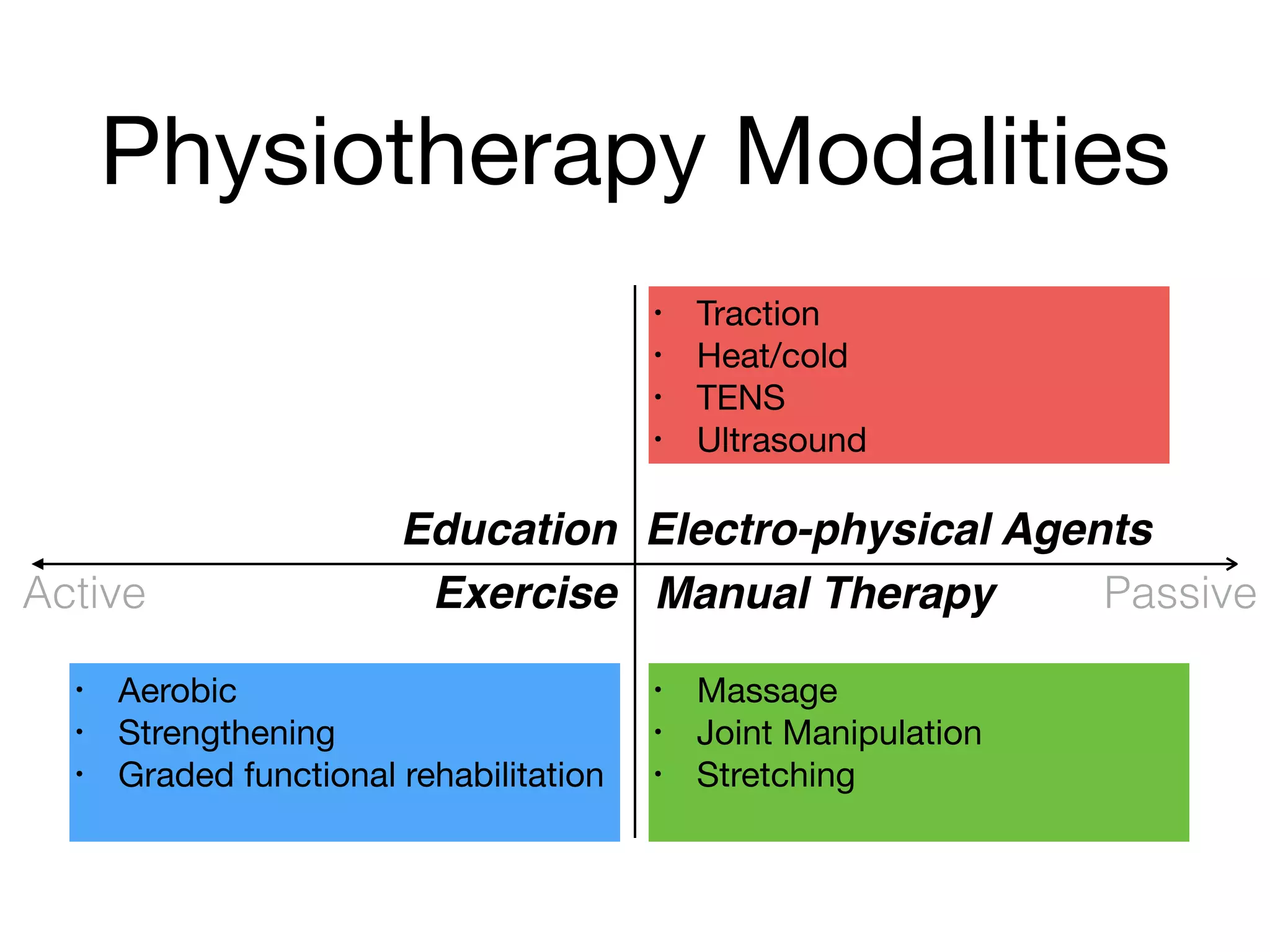
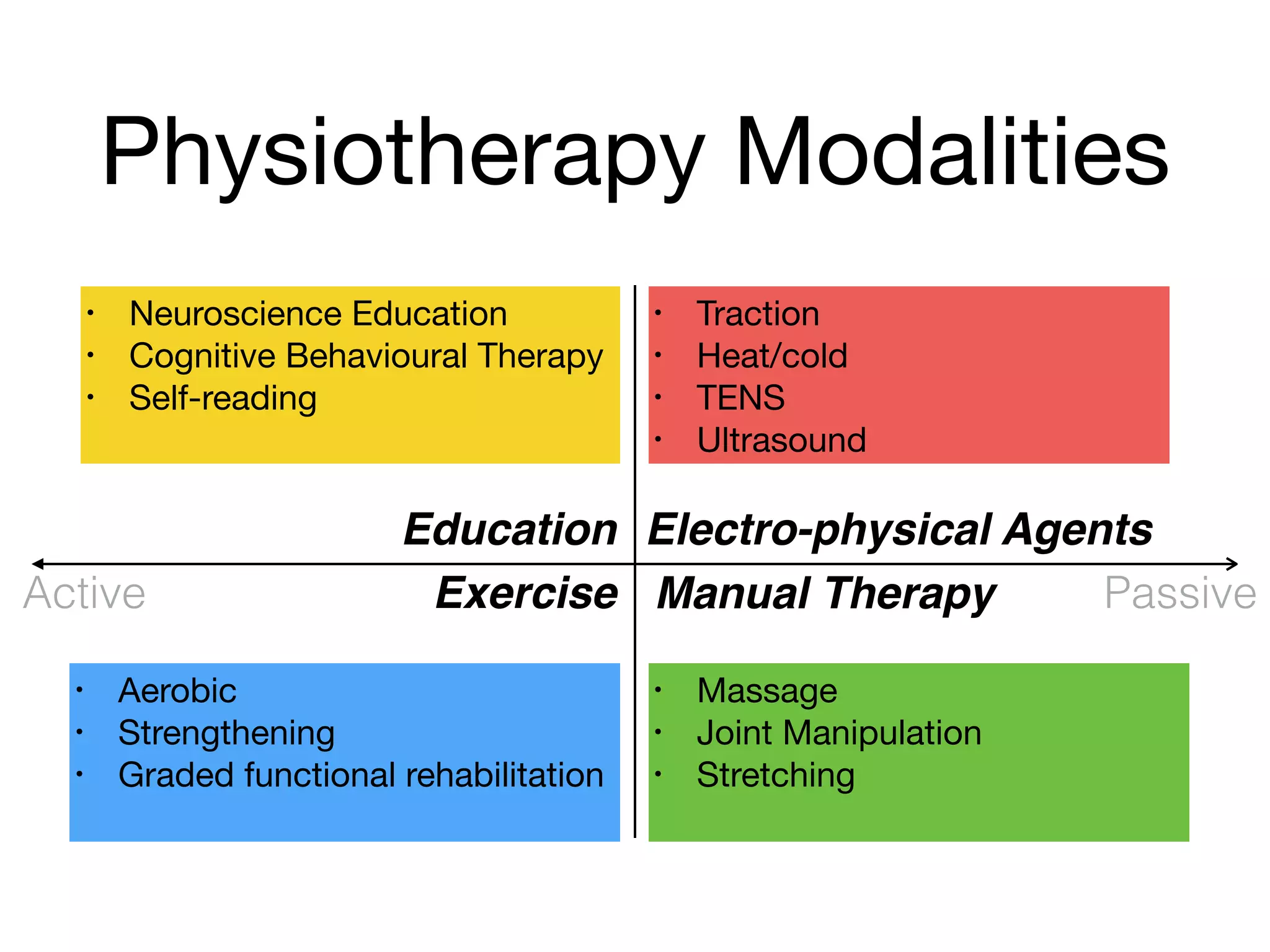
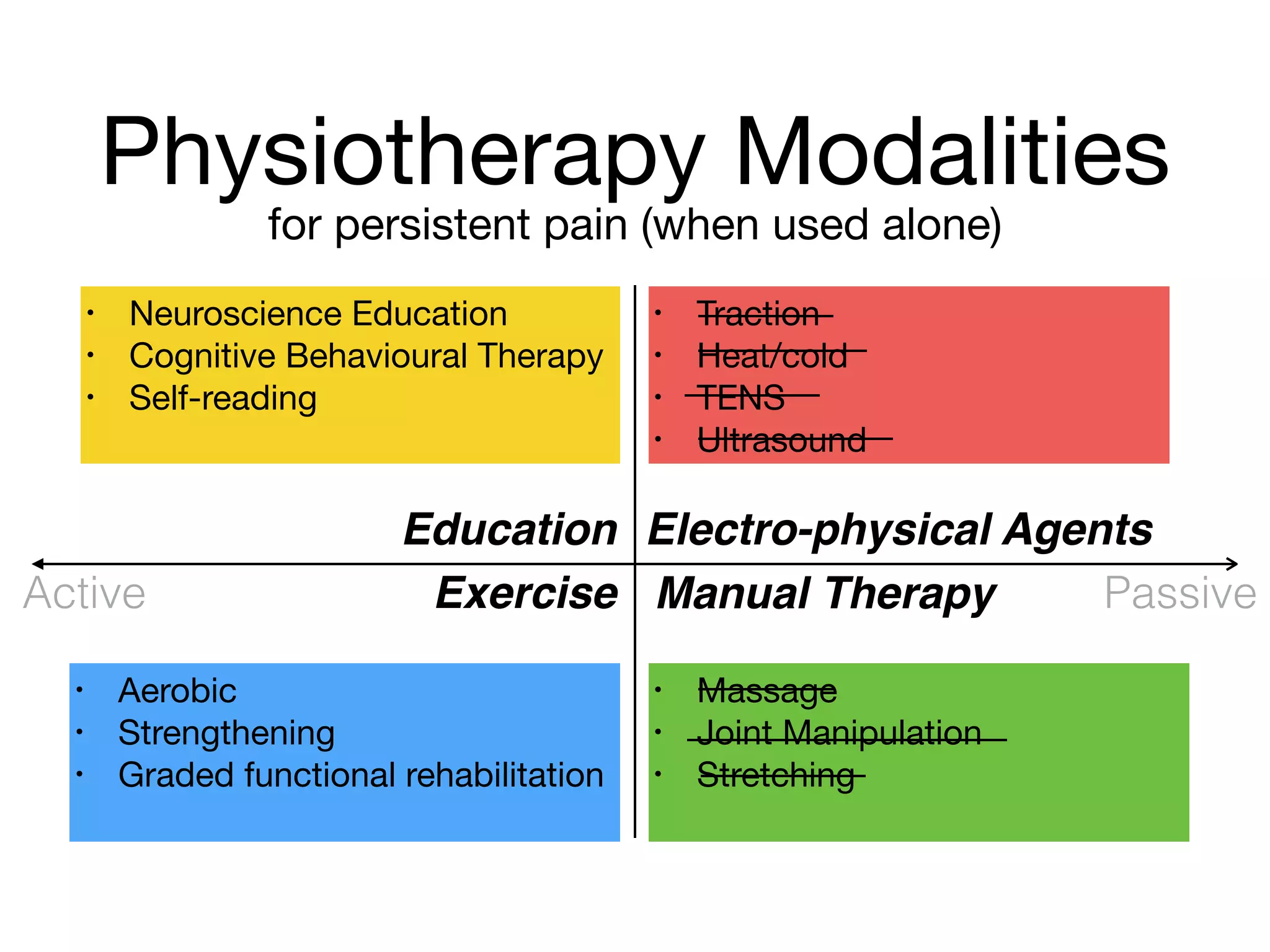
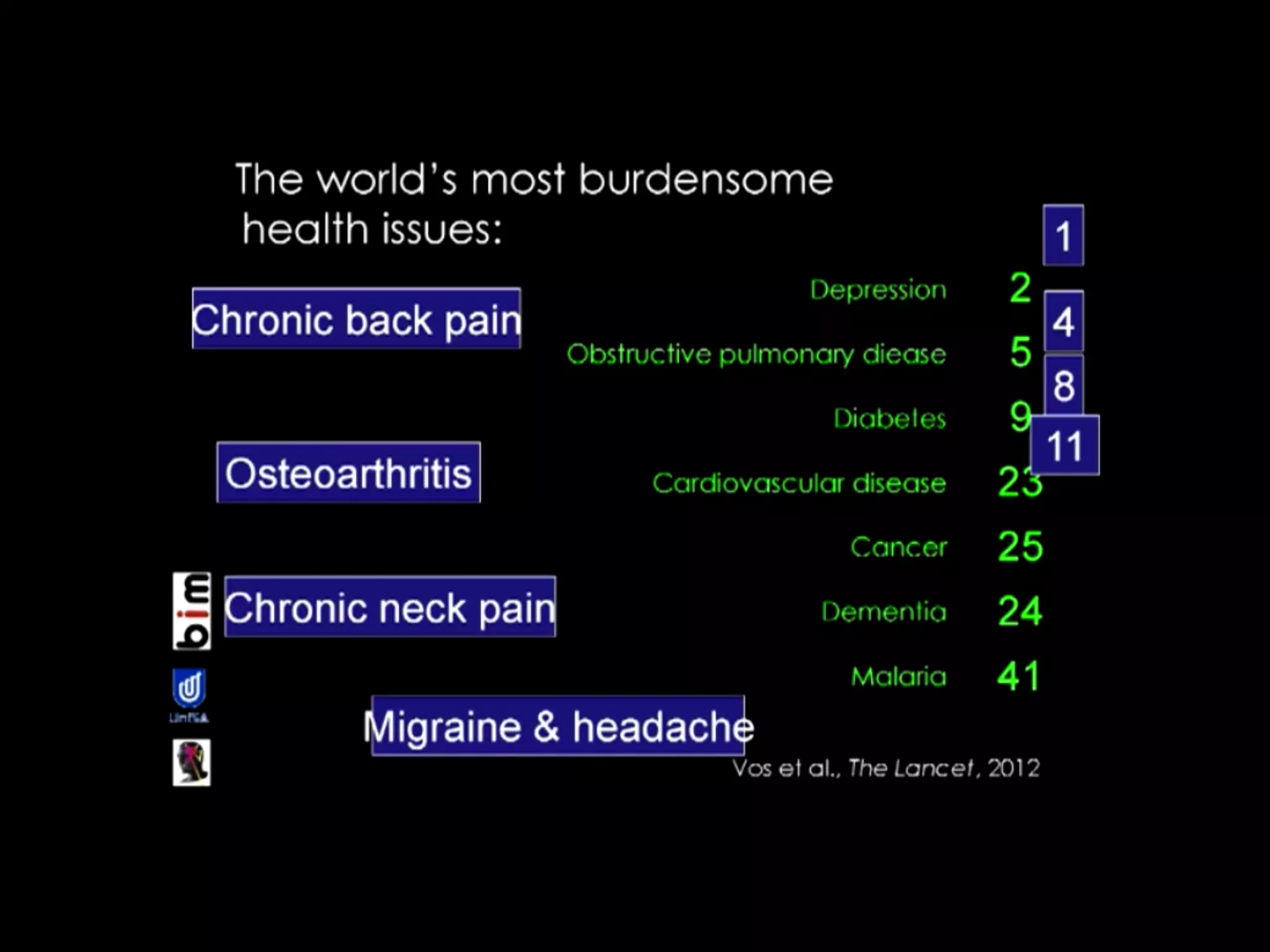
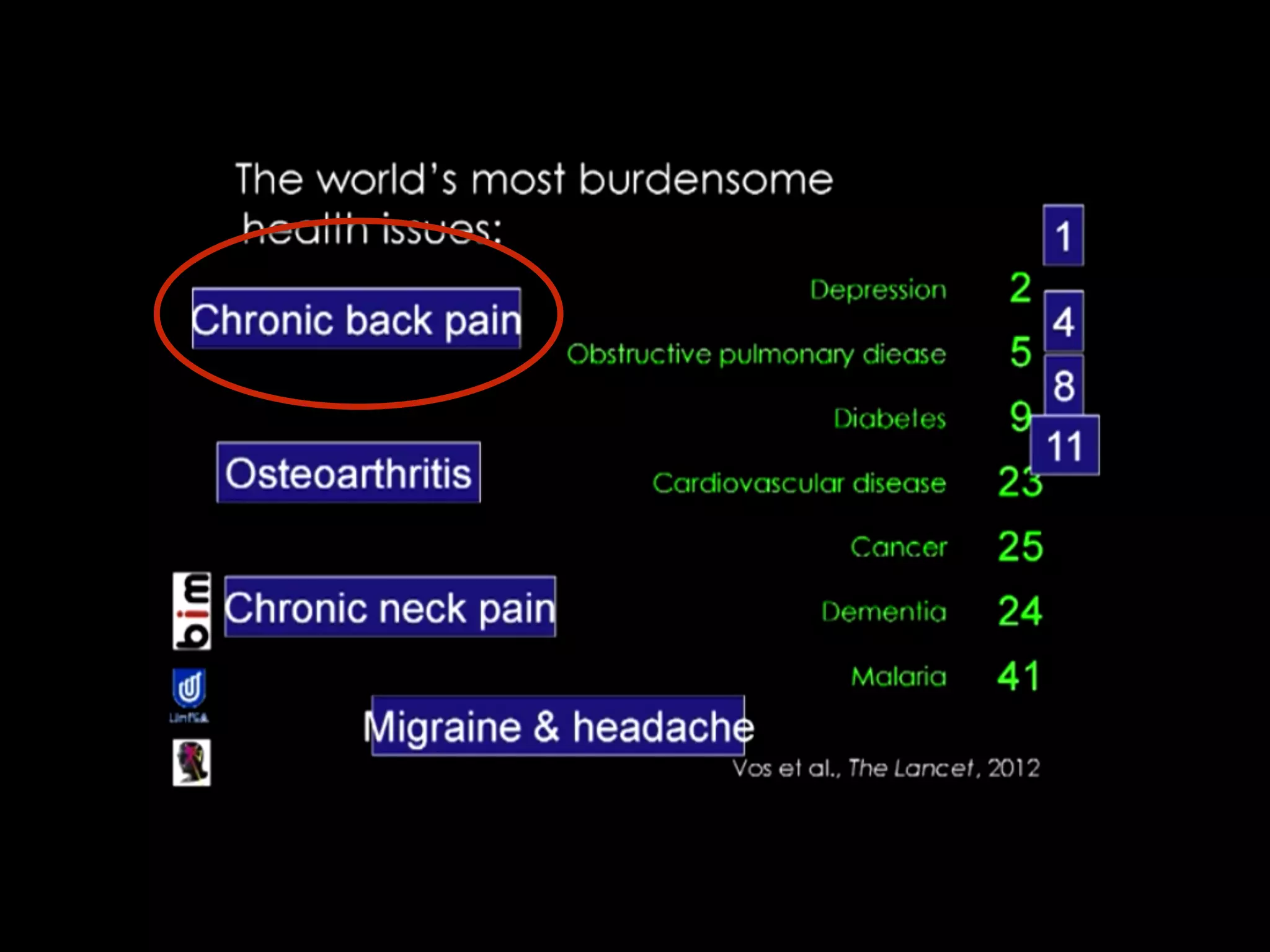
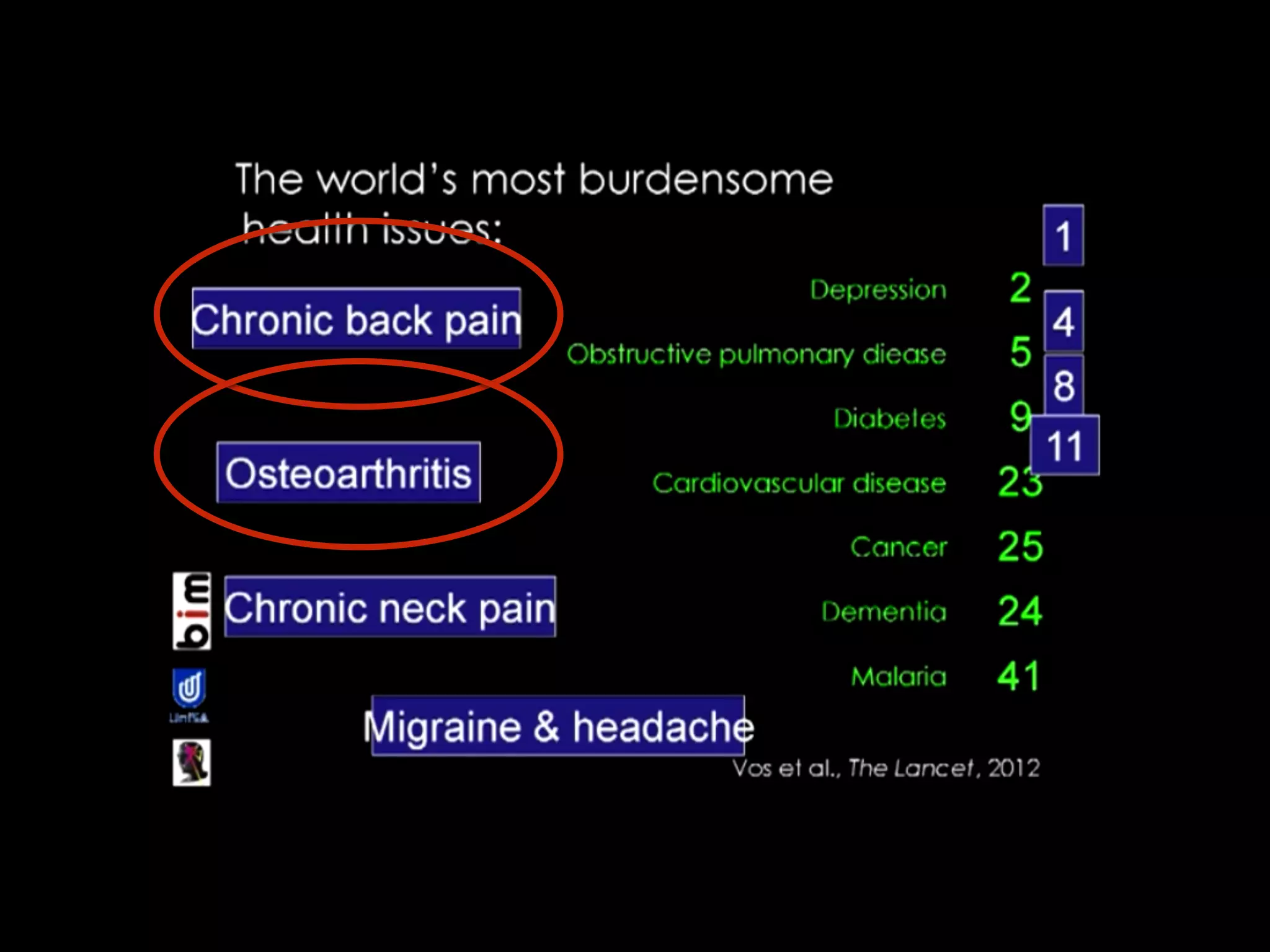
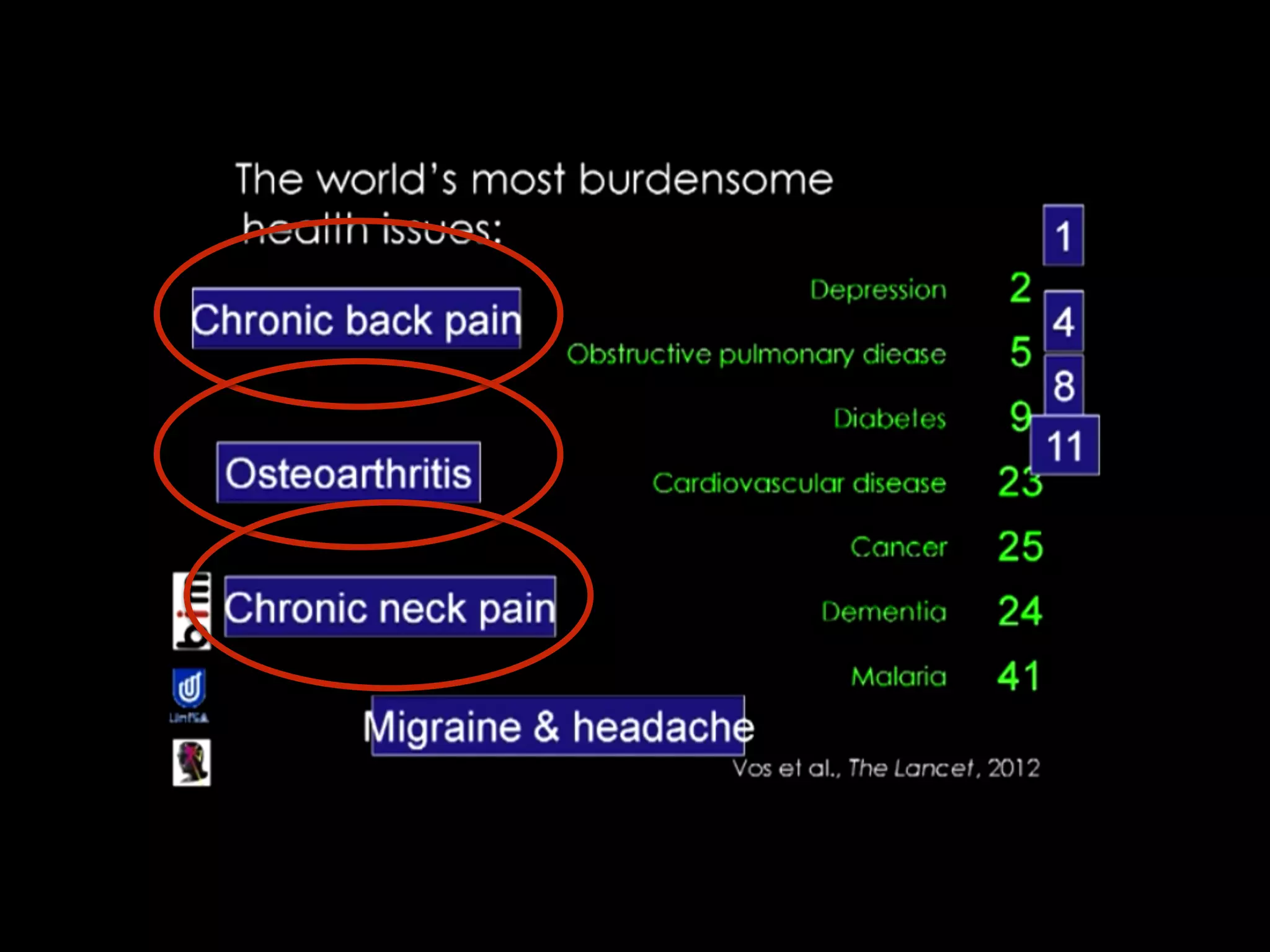
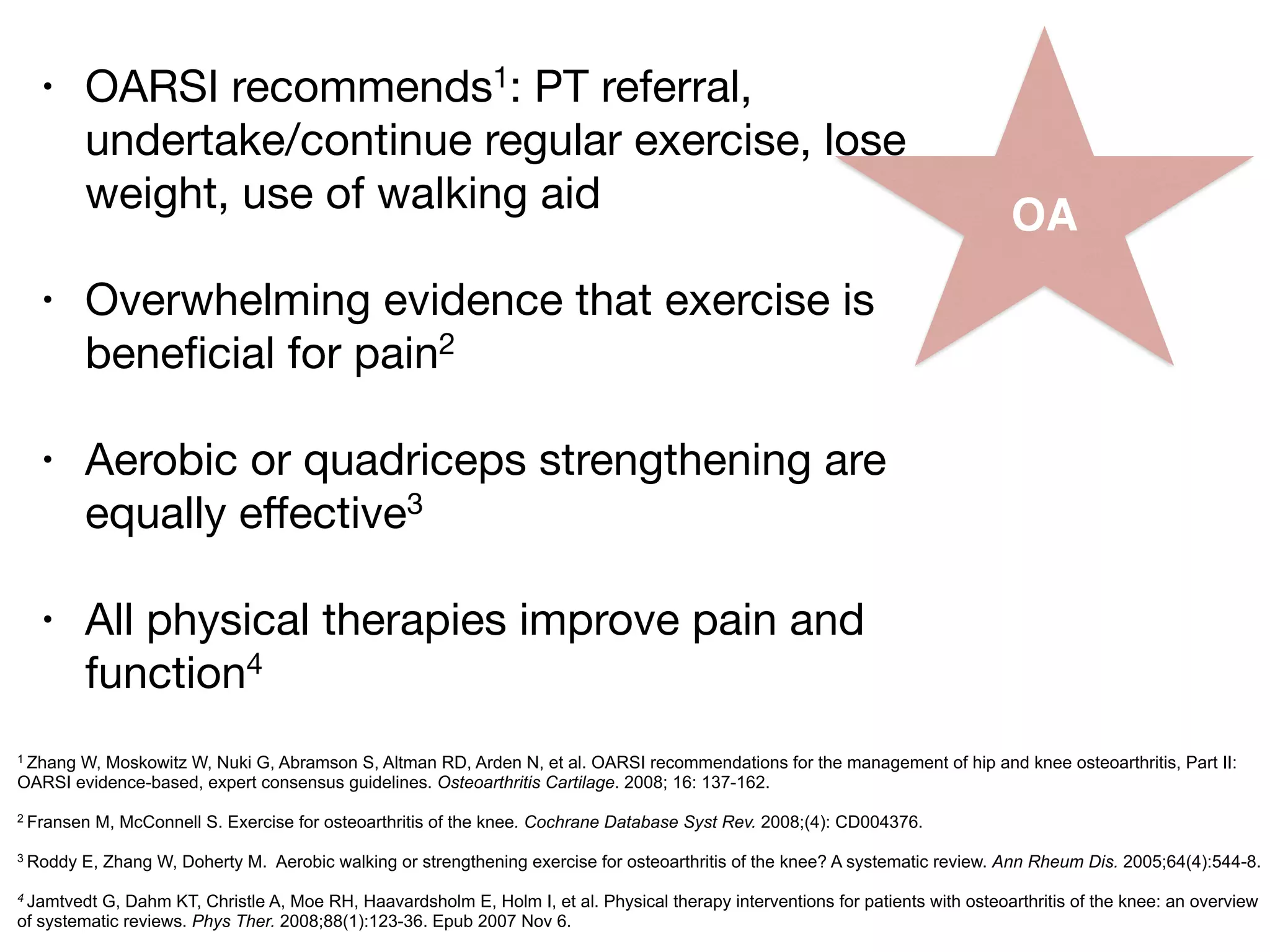
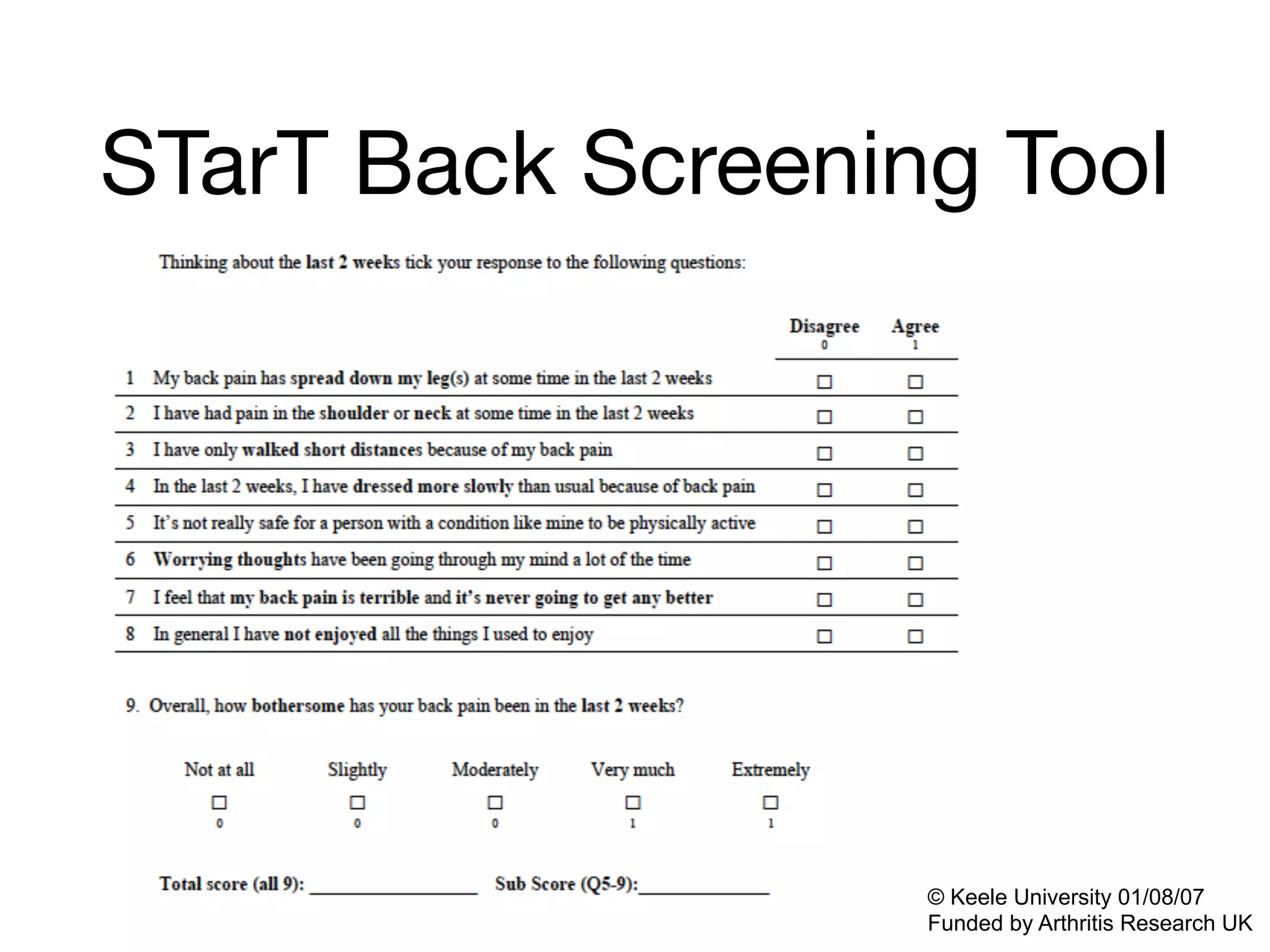
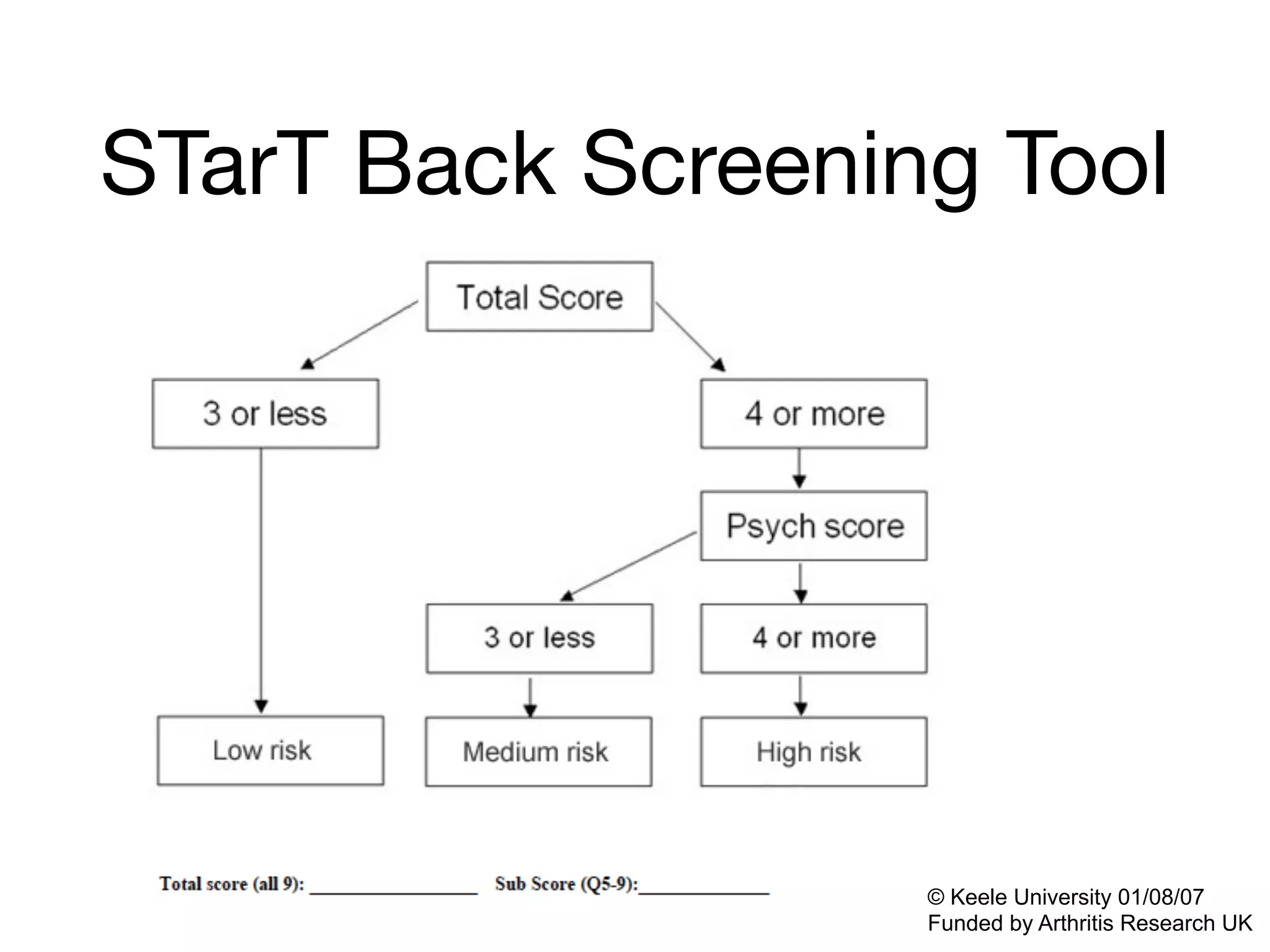
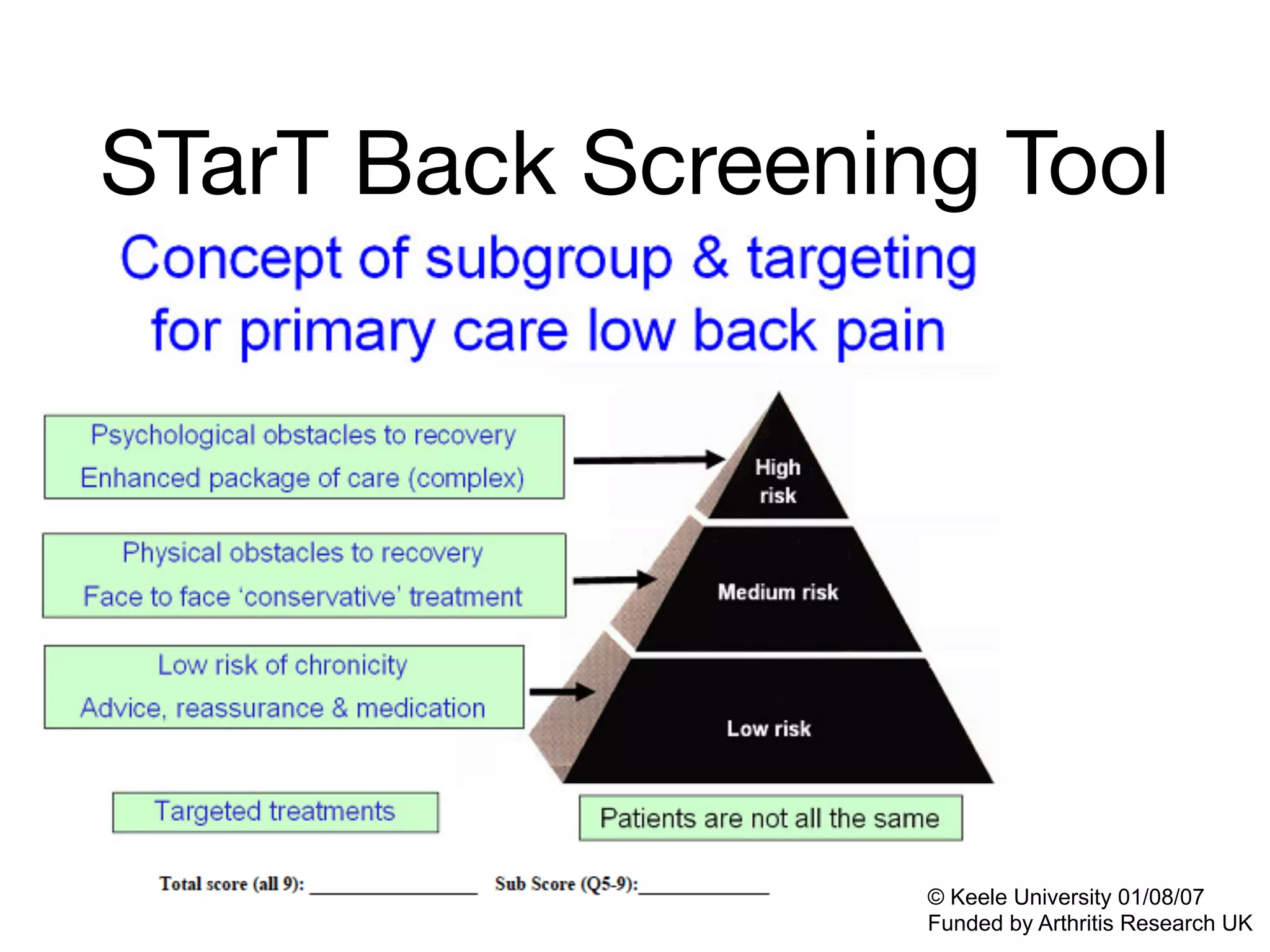
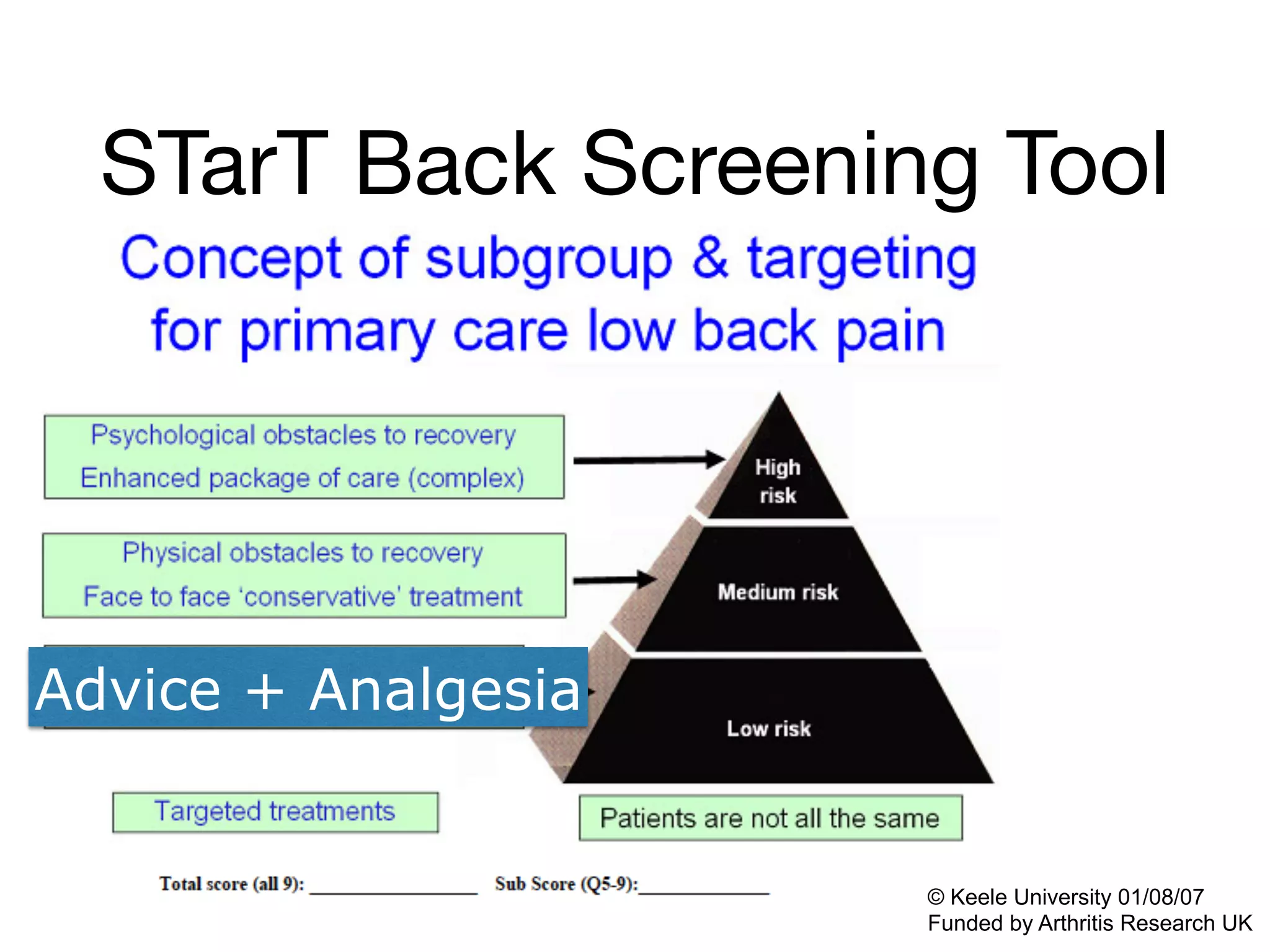
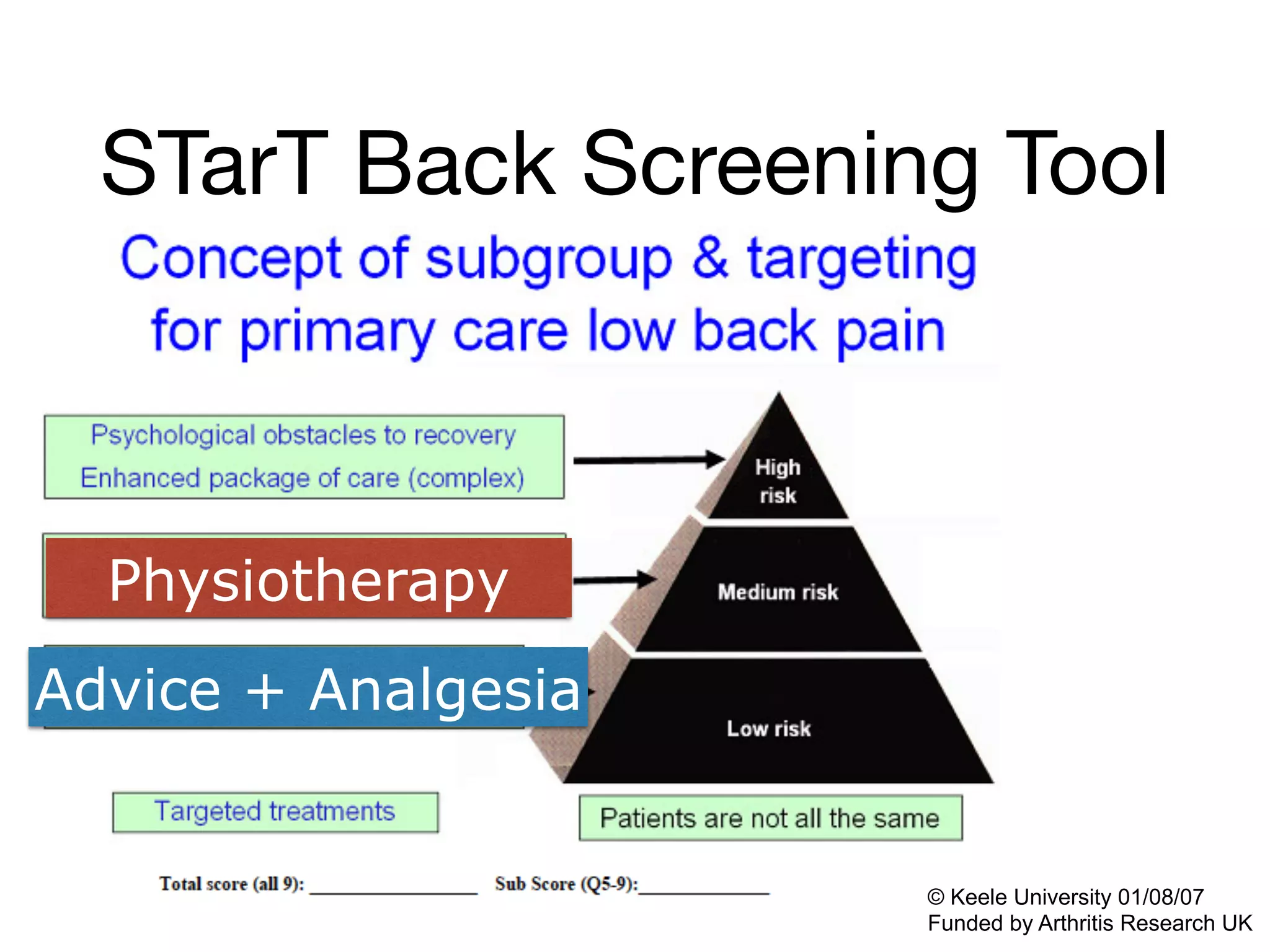
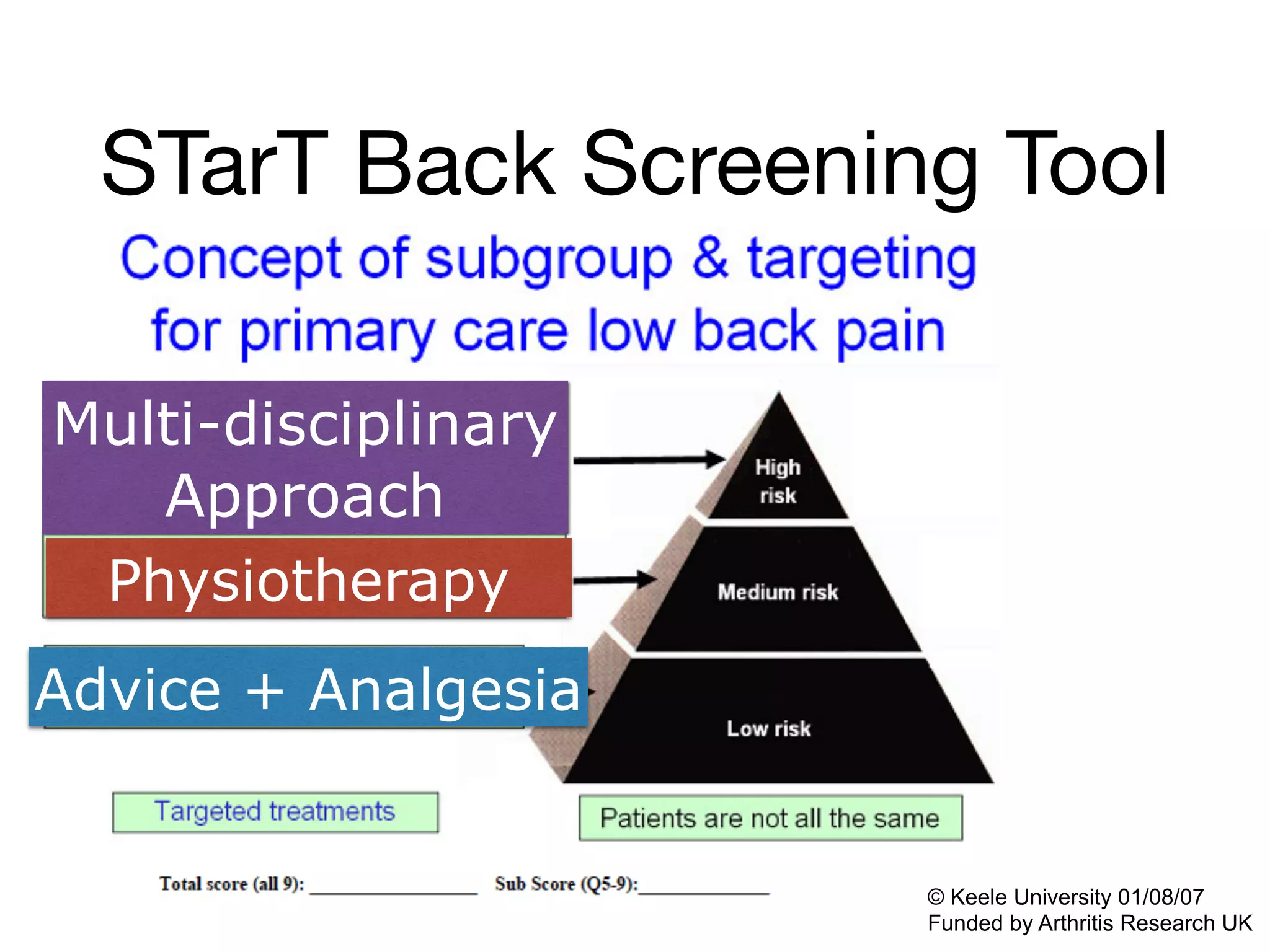
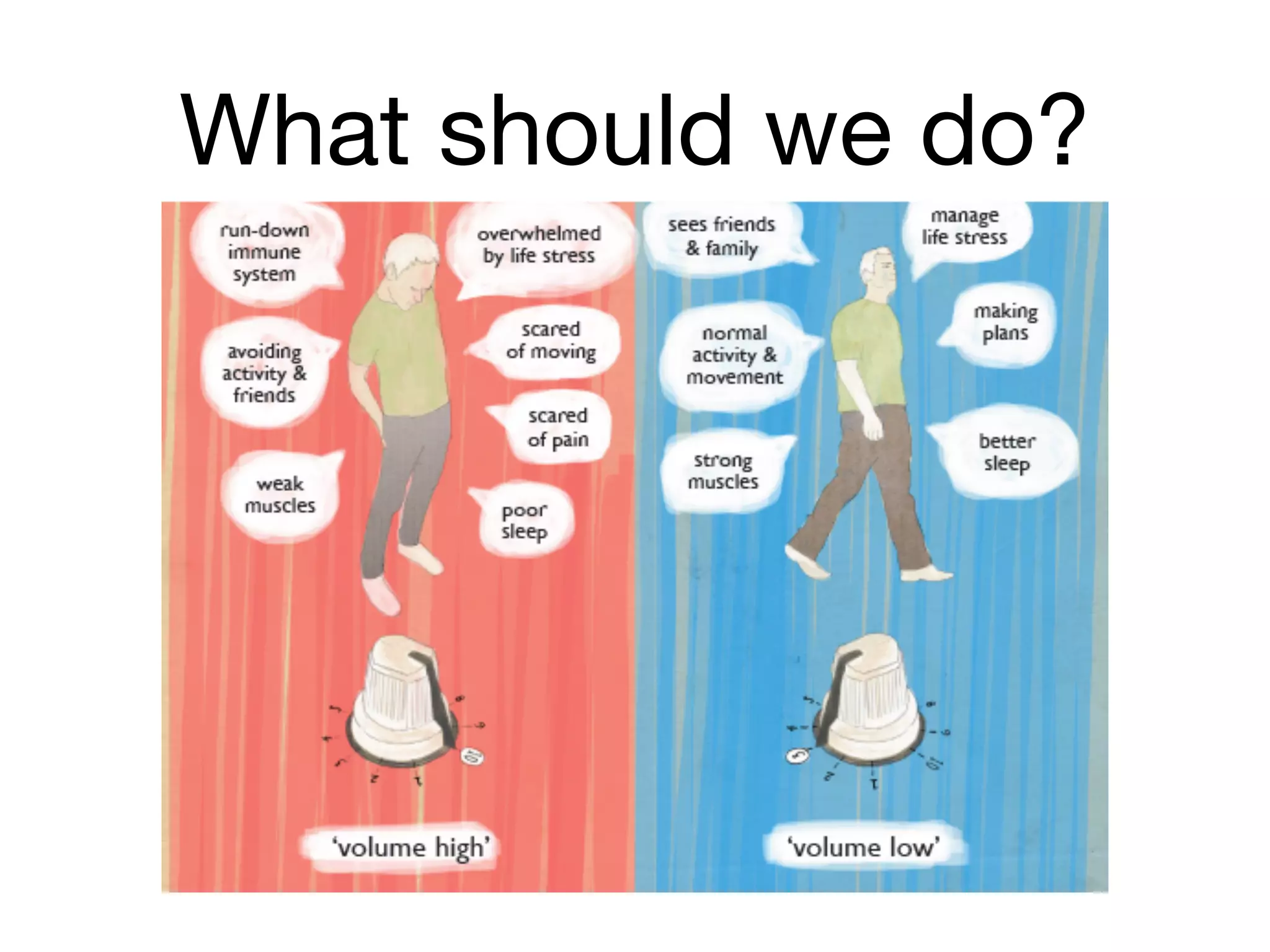



This document summarizes a presentation on physiotherapy for non-cancer chronic pain. It discusses that physiotherapy aims to restore and promote optimal physical function and quality of life for those with persistent pain. It provides an overview of evaluation processes in physiotherapy and various treatment modalities. It also summarizes evidence on approaches for common persistent pain conditions like low back pain, whiplash associated disorder, and osteoarthritis. Screening tools for risk of long-term disability are also briefly covered.















































