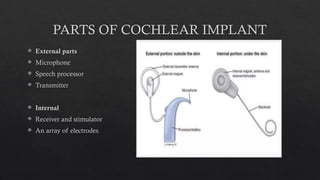
The document outlines the details of cochlear implants, including their components, candidacy criteria, and surgical procedures. Candidates for cochlear implants generally include individuals with severe to profound sensorineural hearing loss who receive little benefit from hearing aids. The document also discusses pre-operative evaluations, potential complications, and the importance of timely implantation for better outcomes.























































![cochlear implant [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cochlearimplantautosaved-230807191245-e9fc2957-thumbnail.jpg?width=640&height=640&fit=bounds)

















![Recent_Advances_Cochlear_Implant_Candidacy_Dr_Anand_Gupta[1]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/recentadvancescochlearimplantcandidacydranandgupta1-1-251128040227-e519dadb-thumbnail.jpg?width=640&height=640&fit=bounds)


























