Downloaded 80 times





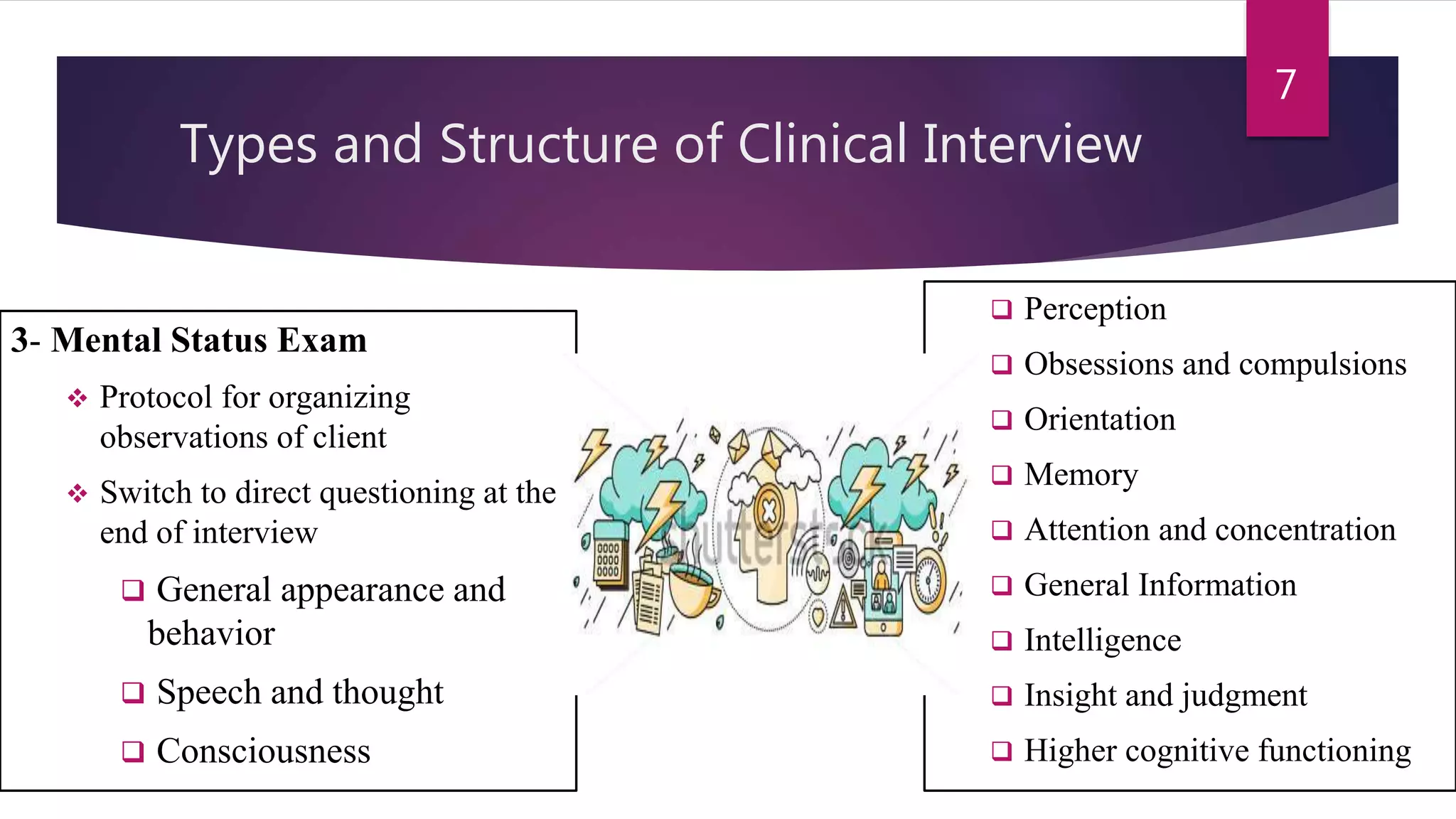


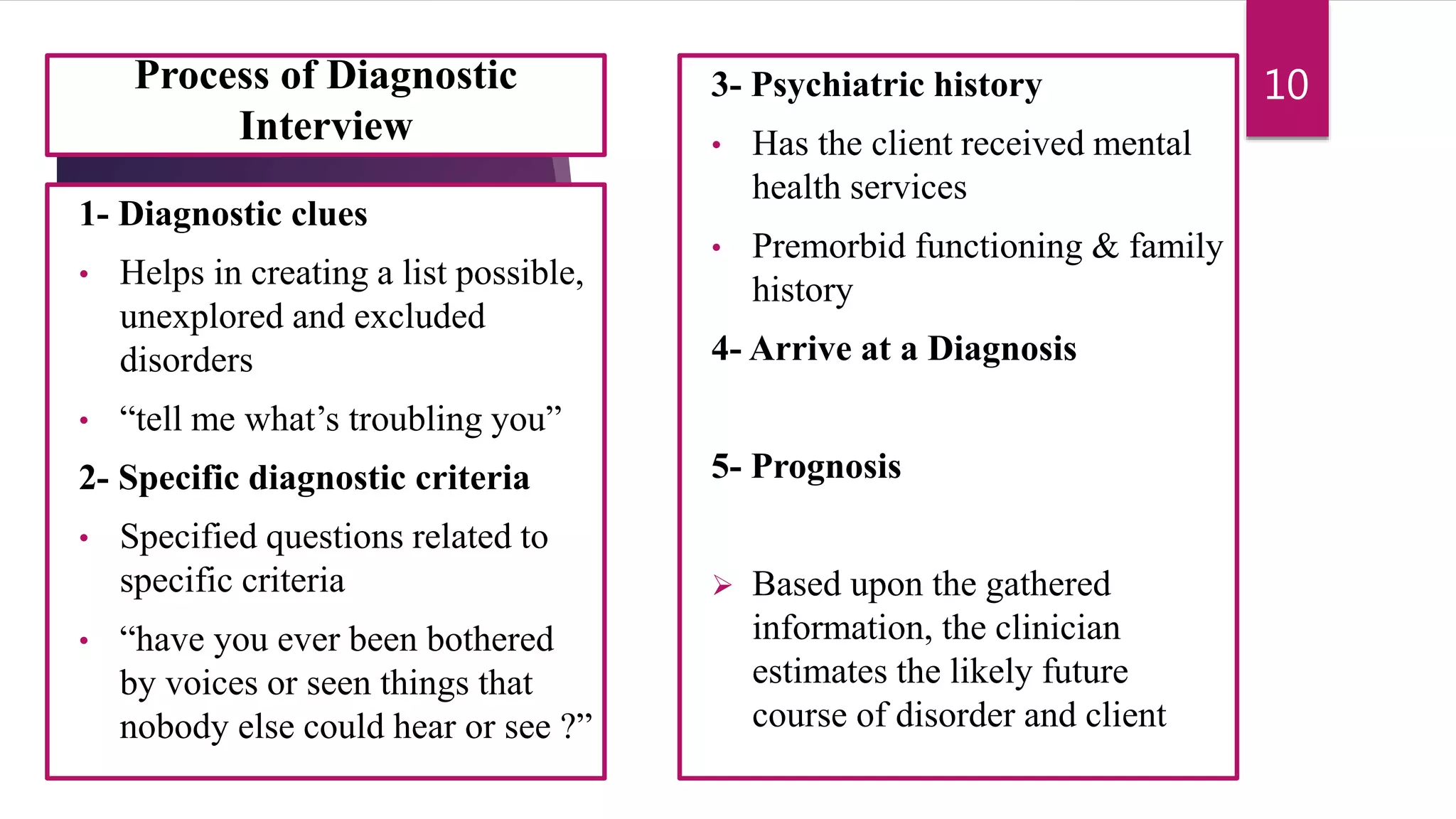






This document provides an overview of the clinical interview process. It discusses the characteristics of a clinical interview, including that it is a one-on-one conversation between a professional and client in a professional setting. It describes the different types and structures of interviews, such as intake interviews, case history interviews, mental status exams, crisis interviews, and diagnostic interviews. Communication strategies for building rapport and conducting the interview are also covered, along with considerations for different populations and common pitfalls.








![Psychodiagnostic technique[1]](https://cdn.slidesharecdn.com/ss_thumbnails/psychodiagnostictechnique1-191031121907-thumbnail.jpg?width=640&height=640&fit=bounds)