
Downloaded 16 times
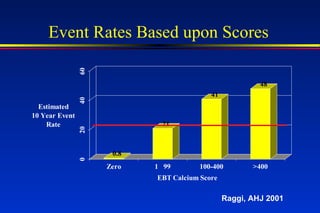
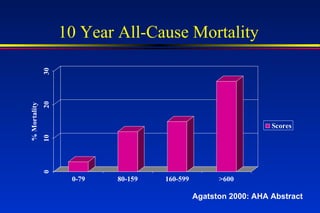
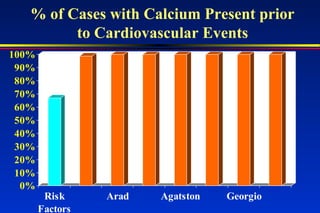
Scores >400 are associated with a 10-fold increased risk of future events. Calcium imaging should be used routinely to identify patients at high risk. Matthew Budoff is an assistant professor who presents on this topic and discloses a relationship with Imatron, Inc. relating to speaking engagements.























































































