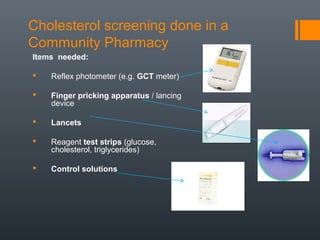
This document provides guidance on screening for cholesterol levels in a community pharmacy setting. It defines cholesterol and hyperlipidemia, outlines who should be screened and how frequently. The summary describes the equipment needed for screening including a photometer, lancing device, test strips, and control solutions. Step-by-step instructions are given for calibrating the photometer, collecting a blood sample via finger prick, running the test strip, and interpreting results. Normal cholesterol ranges are provided along with factors that can influence accuracy.