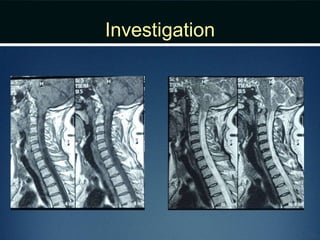
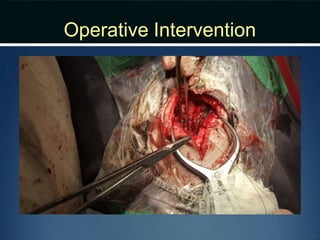
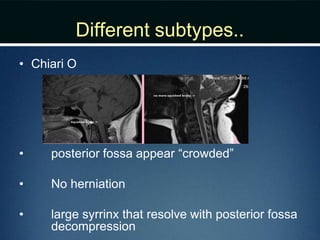
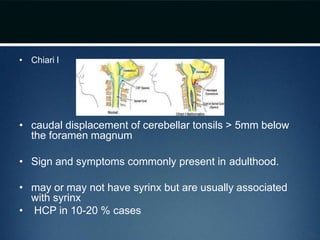
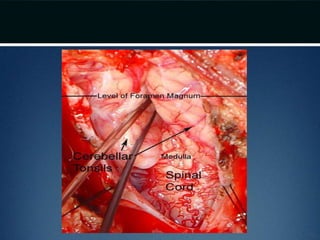
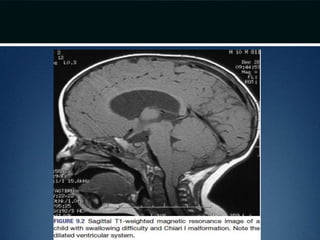
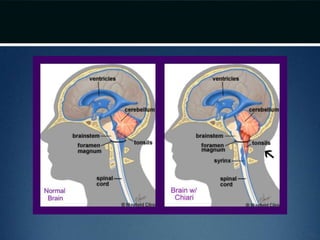
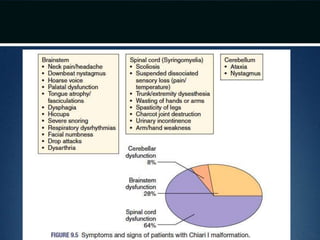
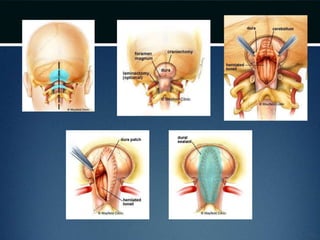
This document describes Chiari malformation, specifically Chiari type I and II. It discusses the presentation, diagnosis, and treatment of a 34-year-old female patient presenting with progressive arm weakness, shoulder pain, and headaches exacerbated by coughing. Examination found reduced sensitivity in her arms. MRI confirmed Chiari type I malformation with tonsillar herniation. The patient underwent posterior fossa decompression surgery, with improvement in symptoms at 6-month follow up. Chiari malformations cause hindbrain herniation and obstruction of CSF flow, often requiring surgery to enlarge the posterior fossa.