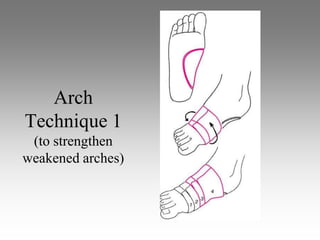
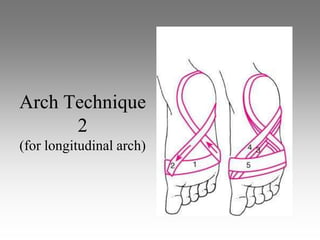
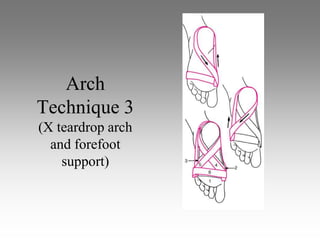
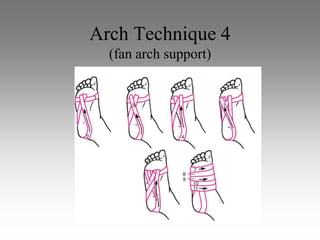
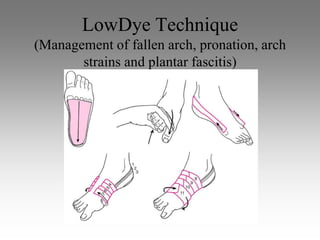
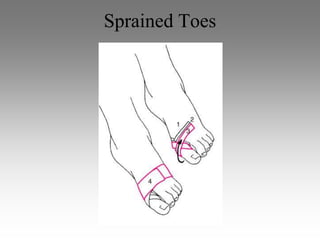
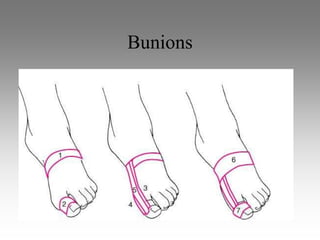
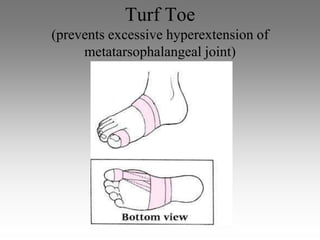
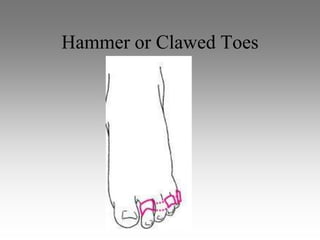
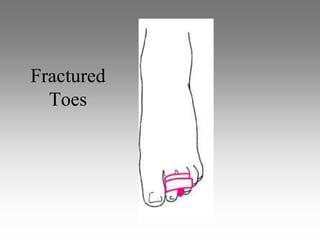
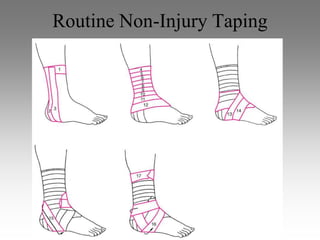
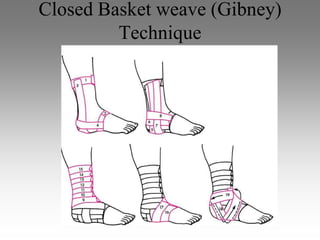
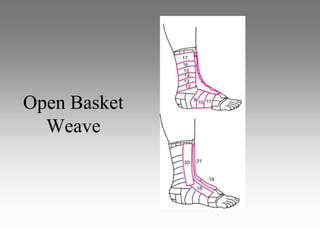
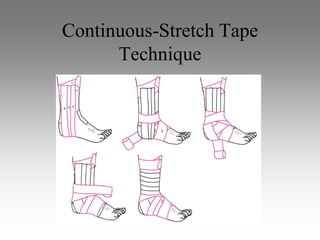
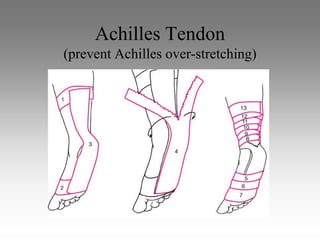
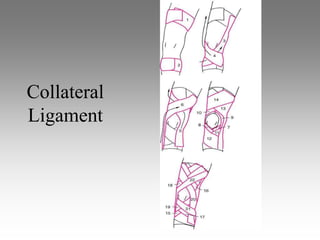
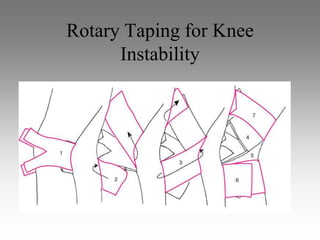
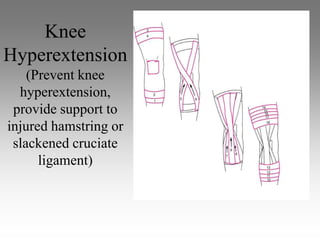
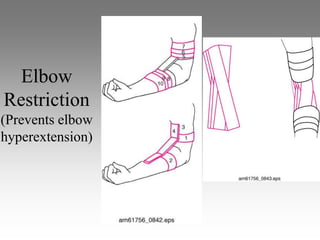
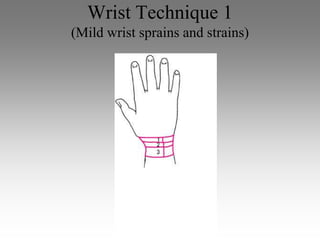
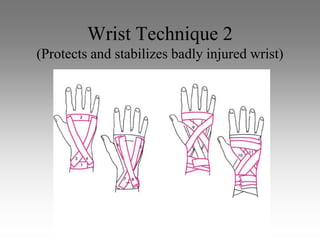
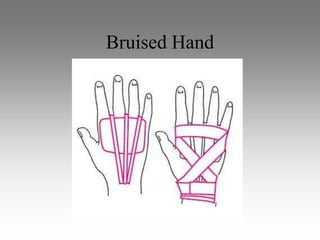
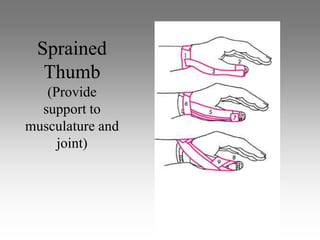
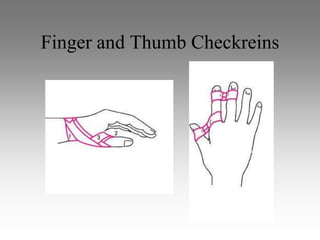
Bandaging and taping are important techniques for injury management and prevention. A variety of materials like gauze, cotton cloth, and elastic bandages can be used for bandaging, with application requiring firm but not restrictive pressure. Taping uses materials like non-elastic and elastic tapes, with proper techniques involving overlapping strips and contouring to the body. Common bandaging and taping procedures are described for the foot, ankle, knee, elbow, wrist, and fingers to provide support and stabilization for injuries.