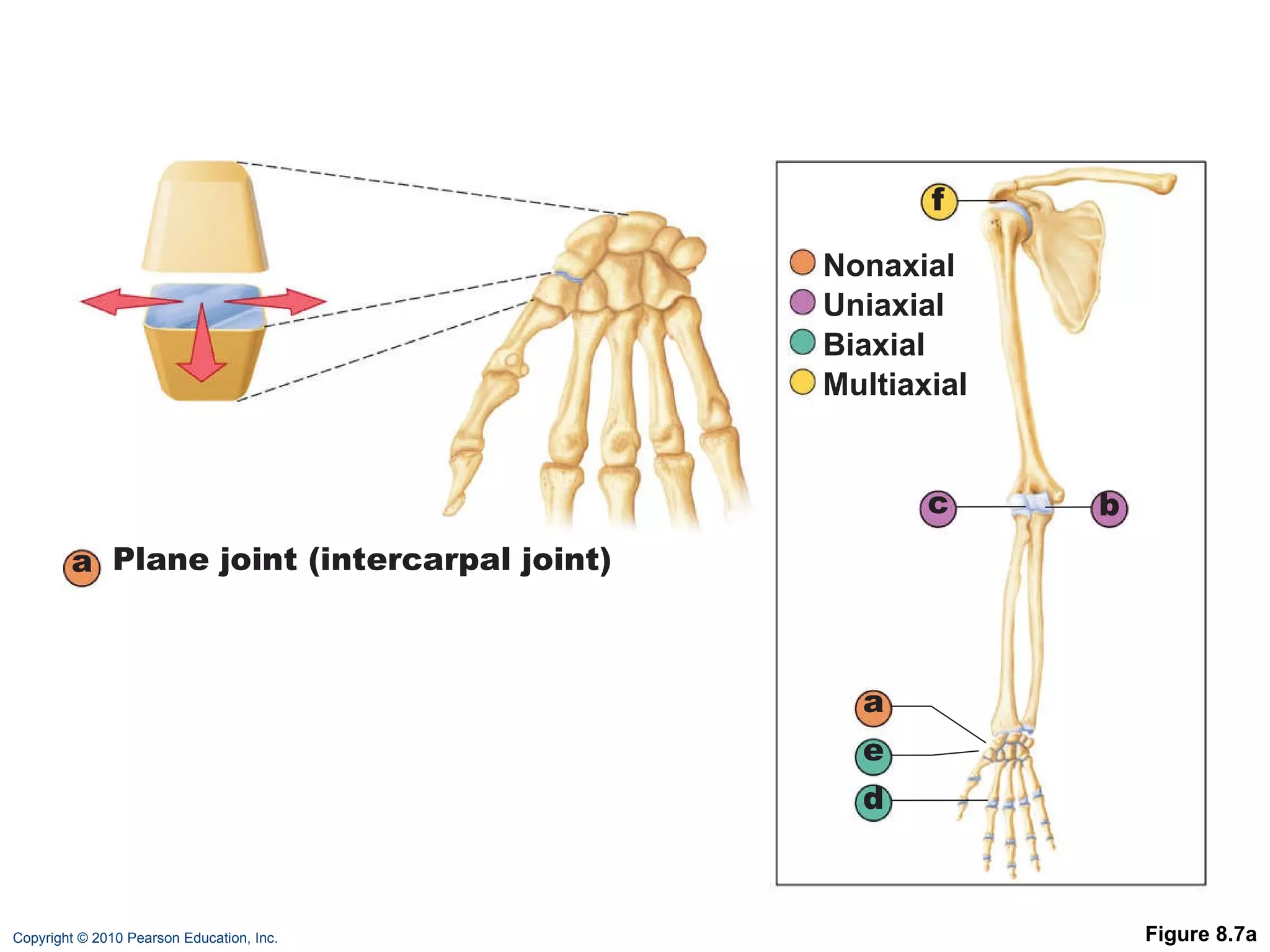
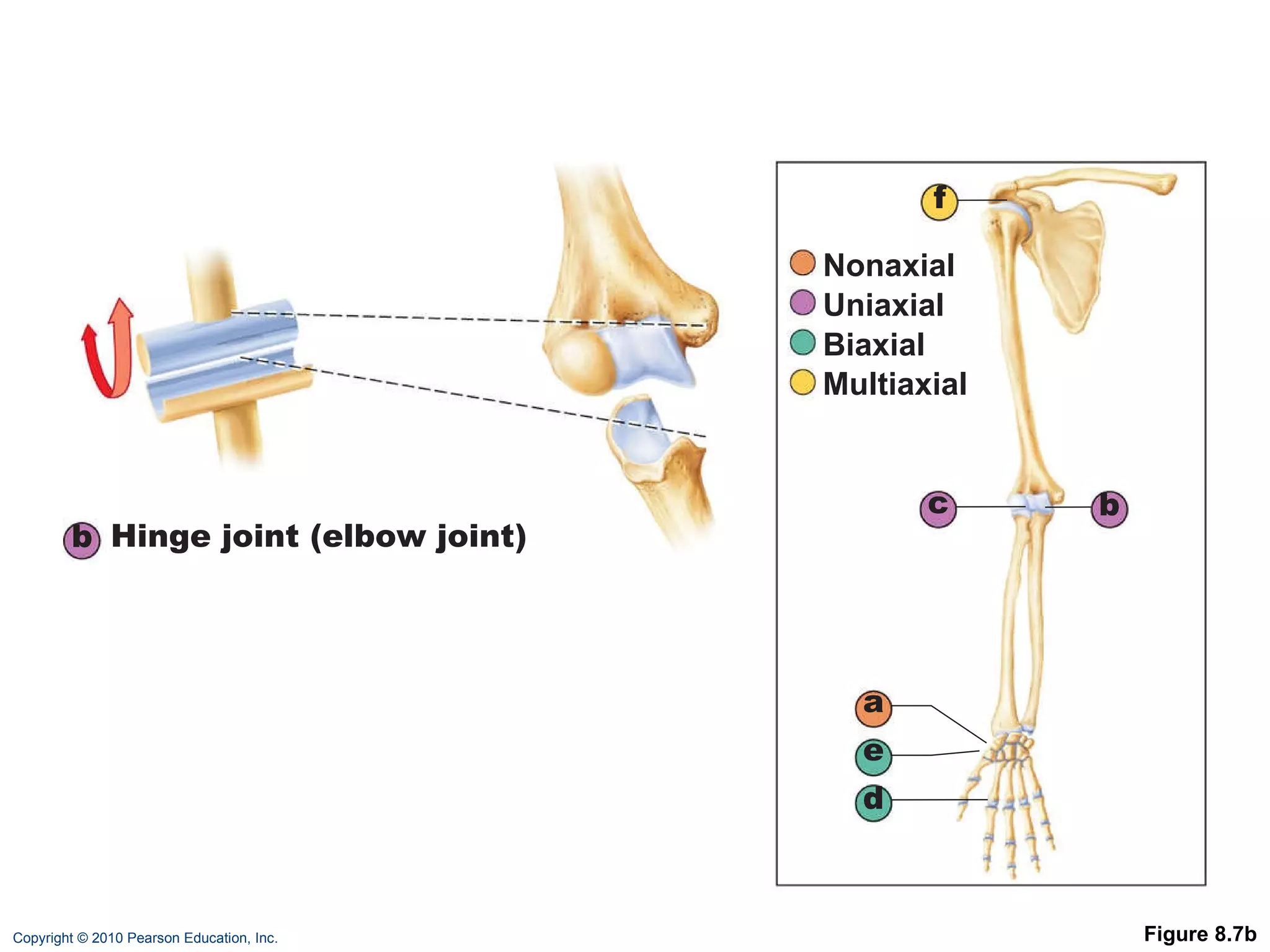
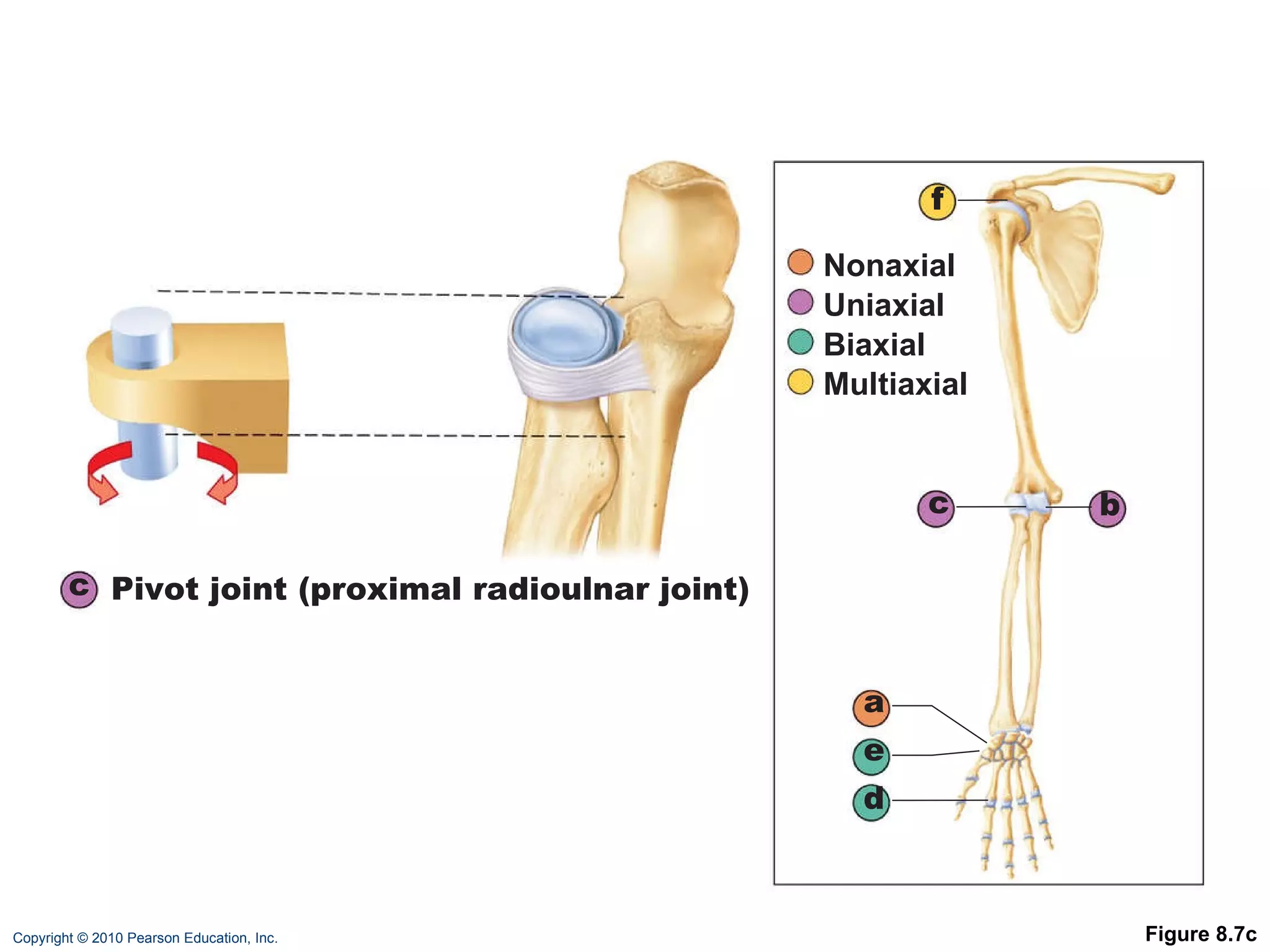
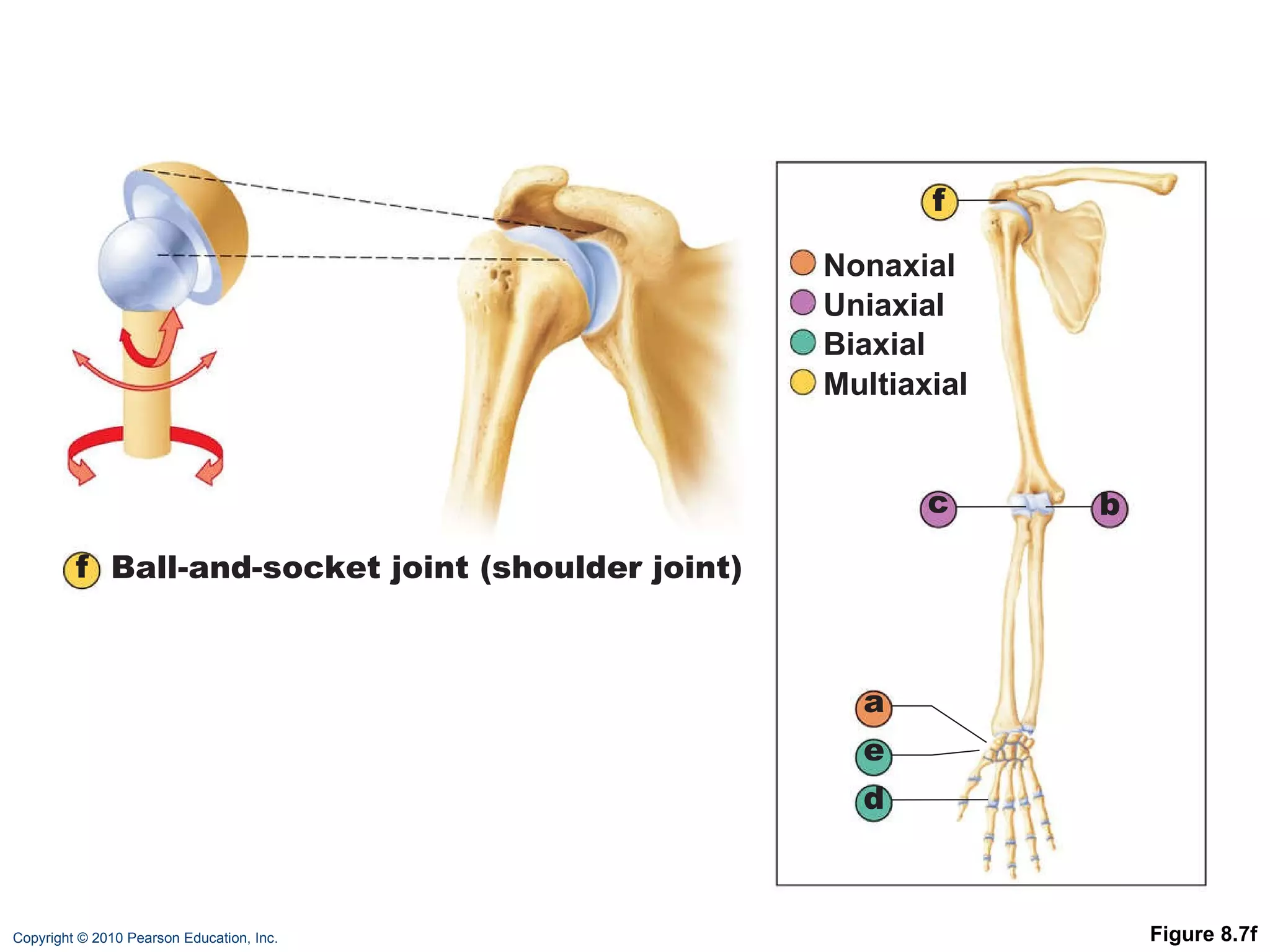
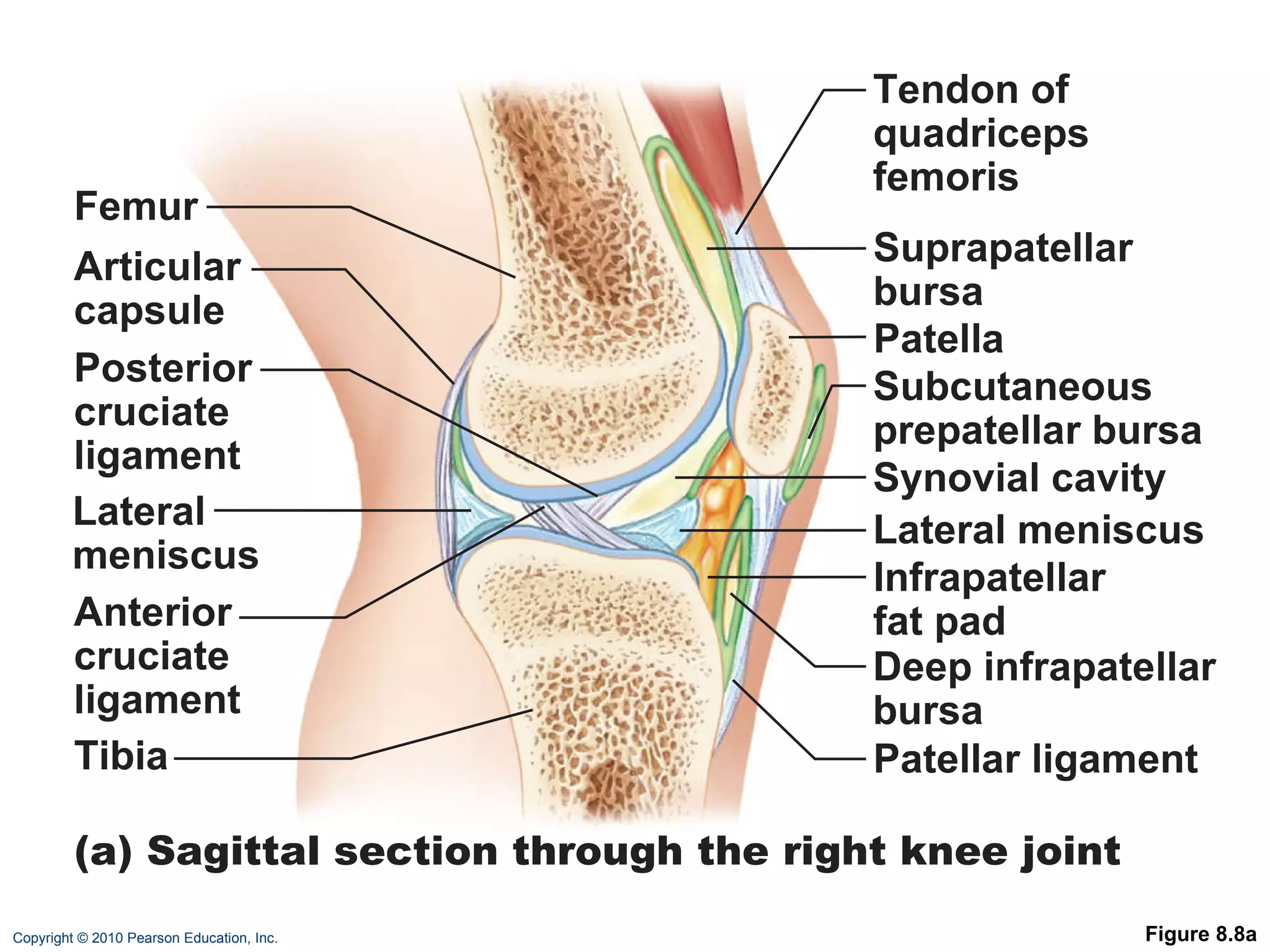
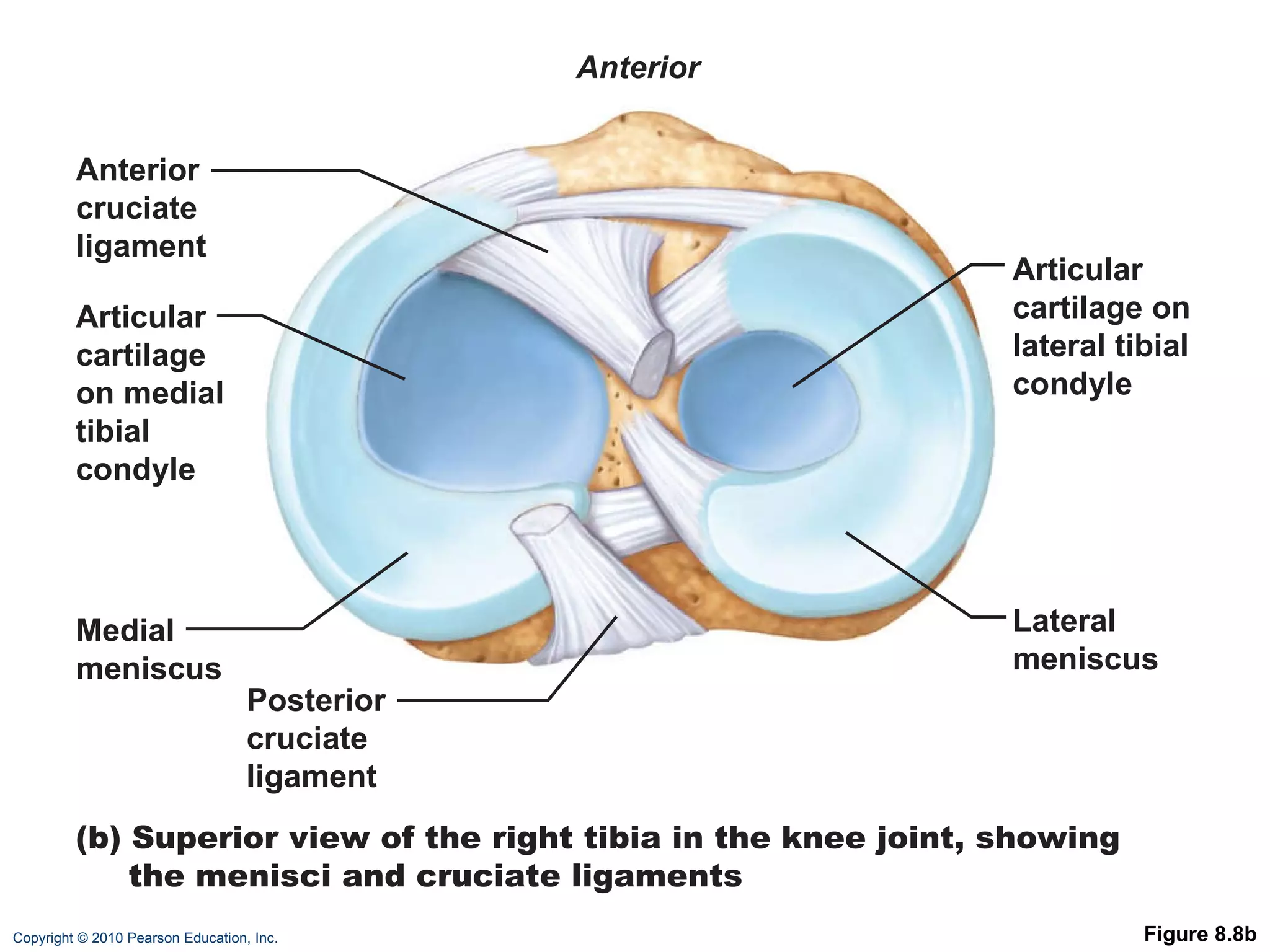
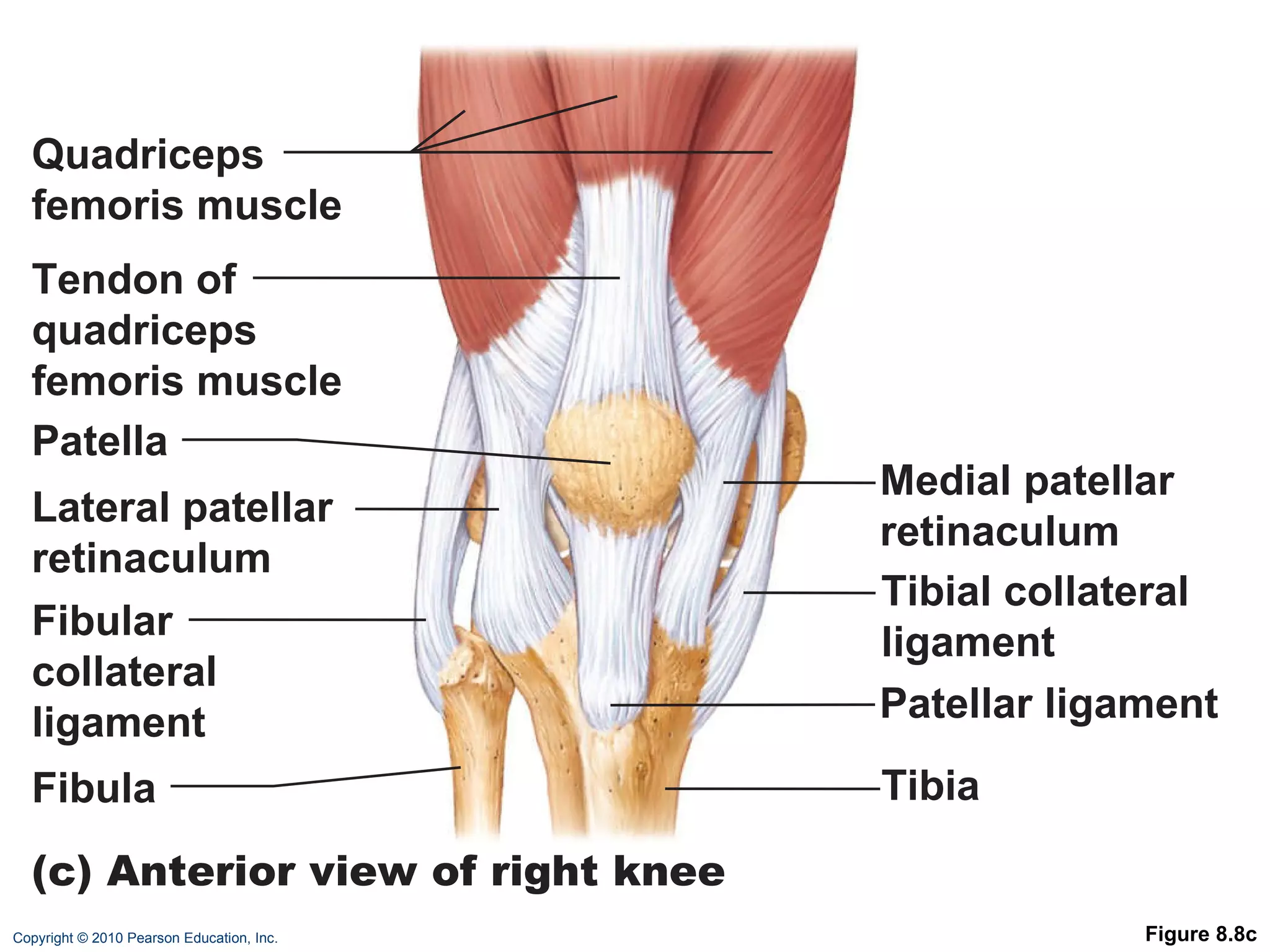
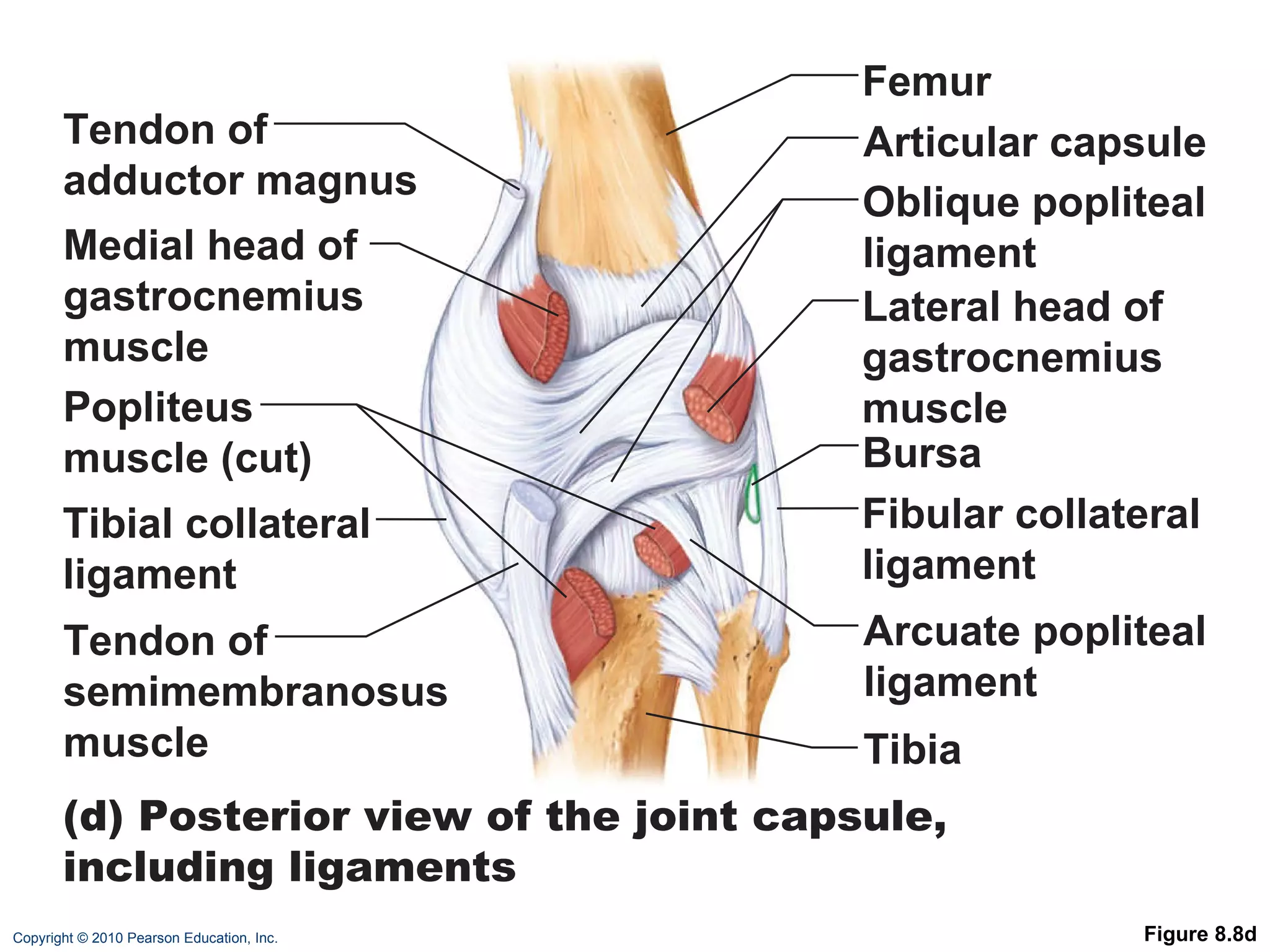
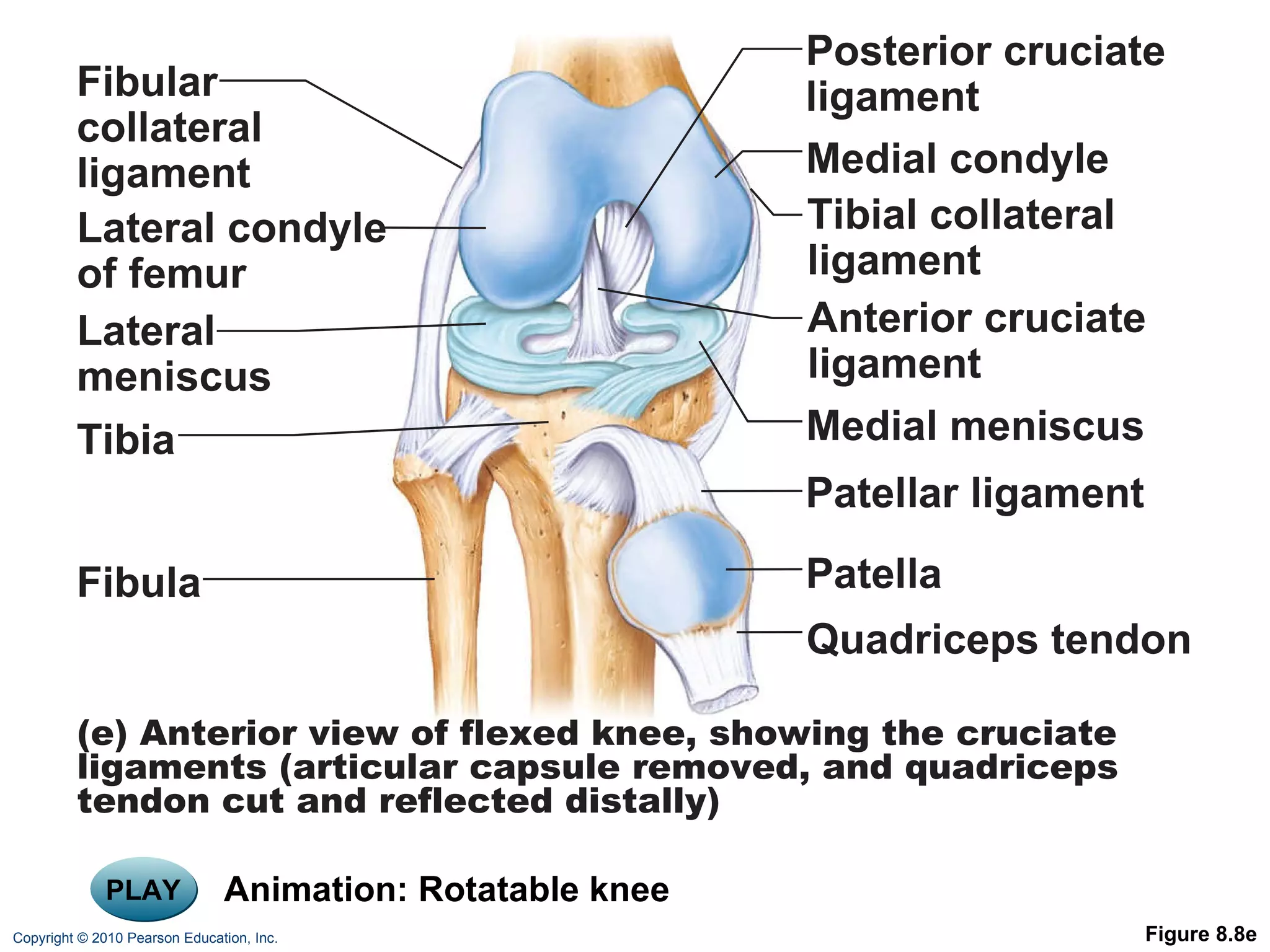
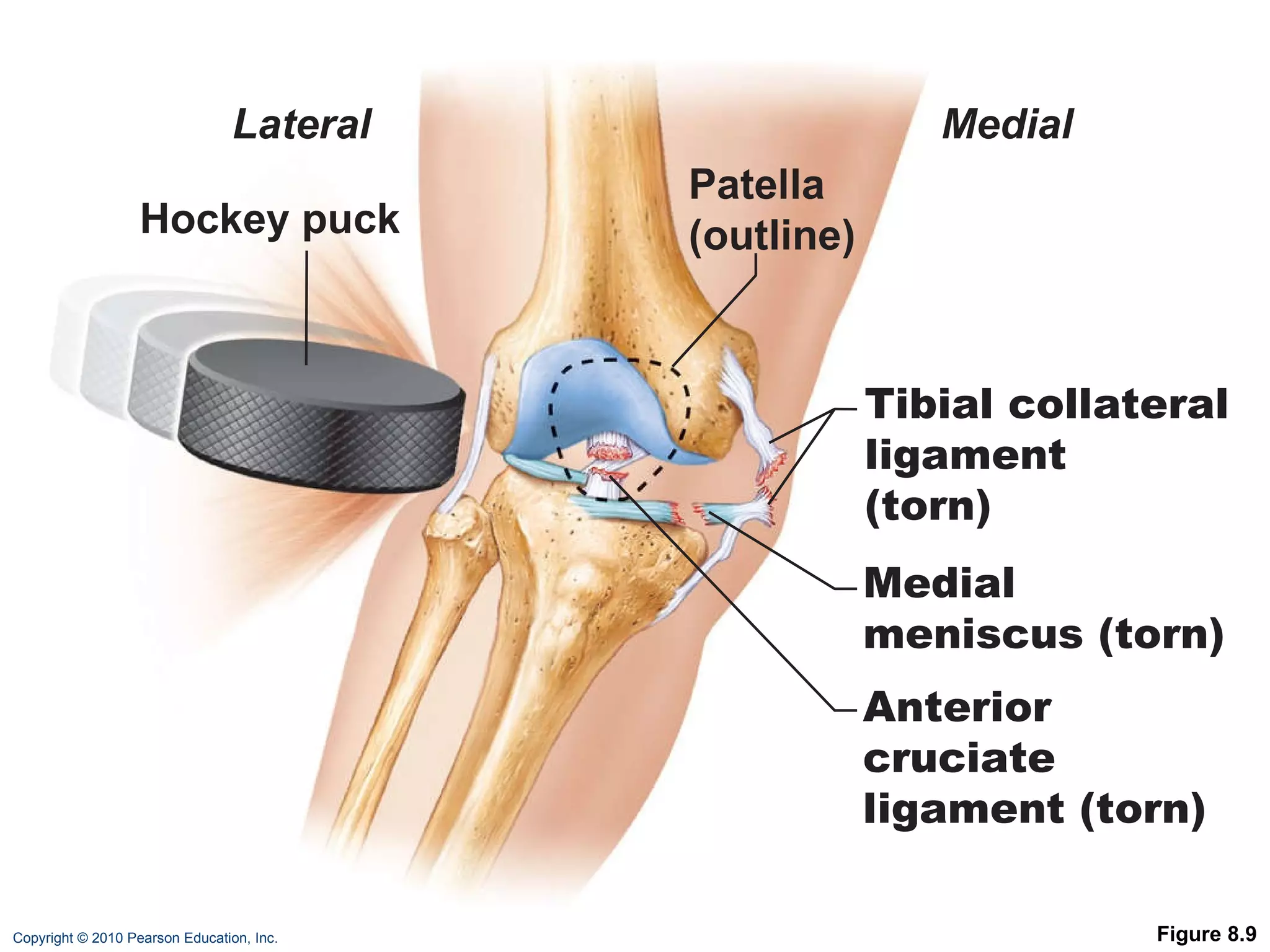
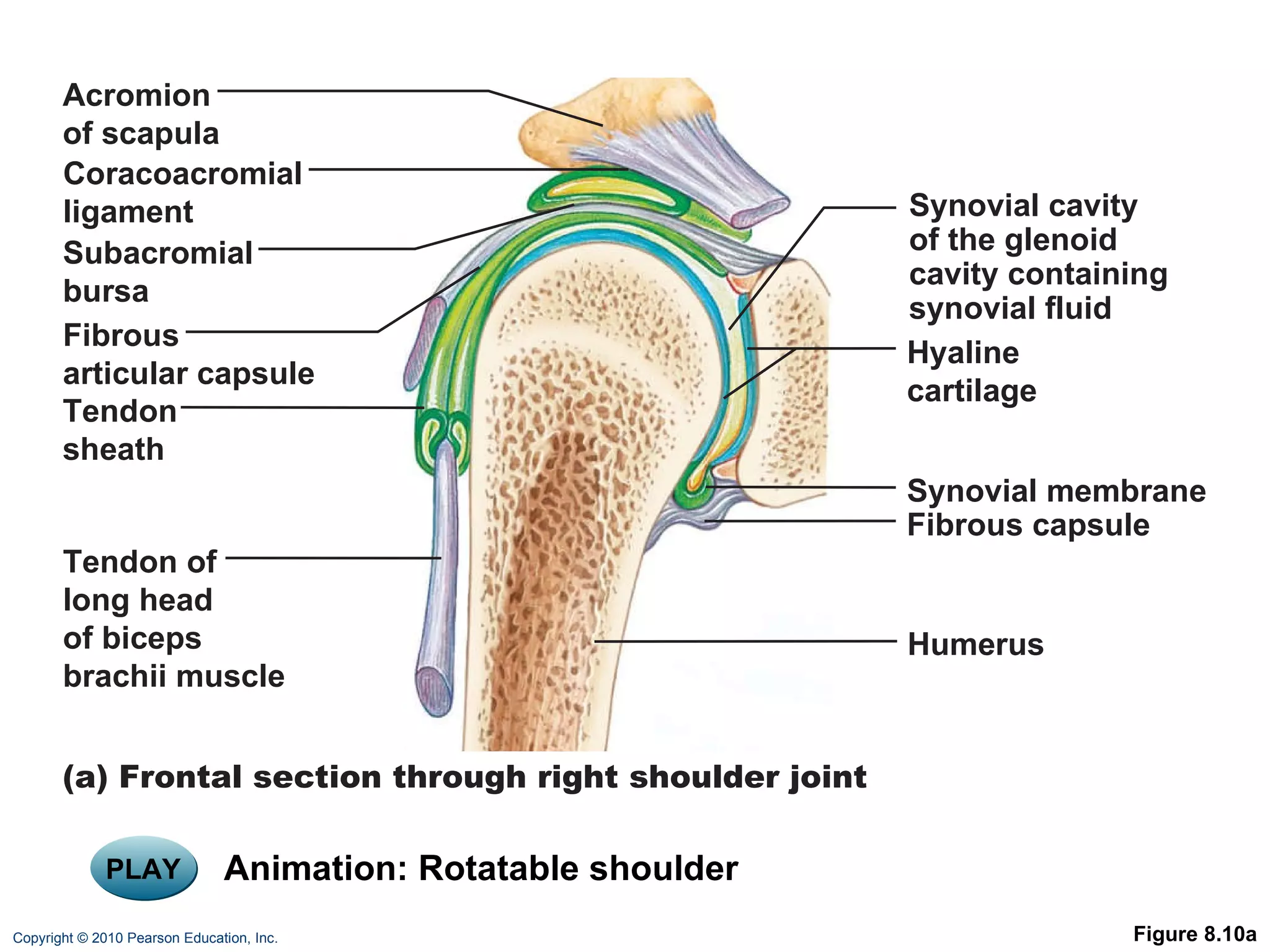
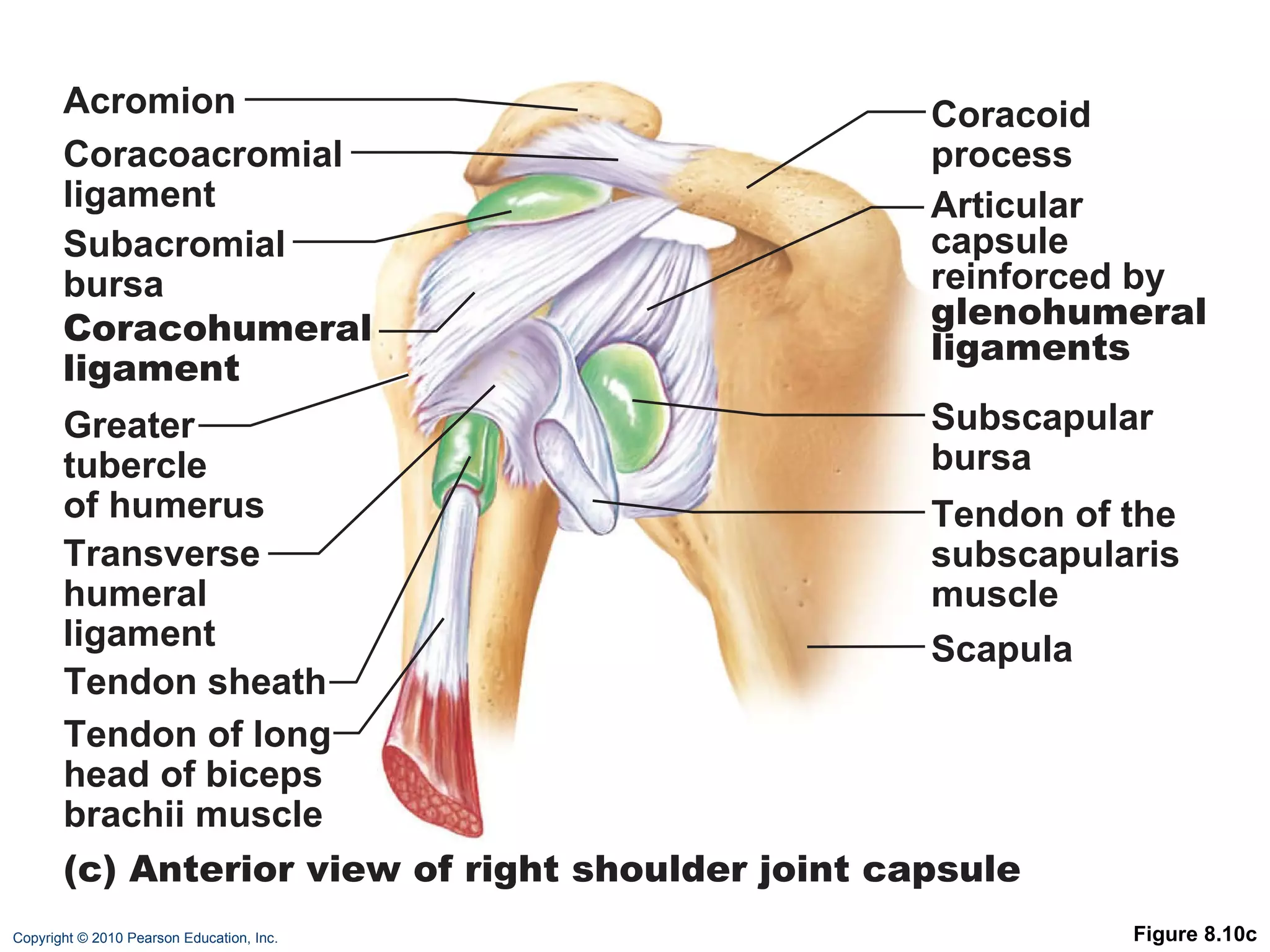
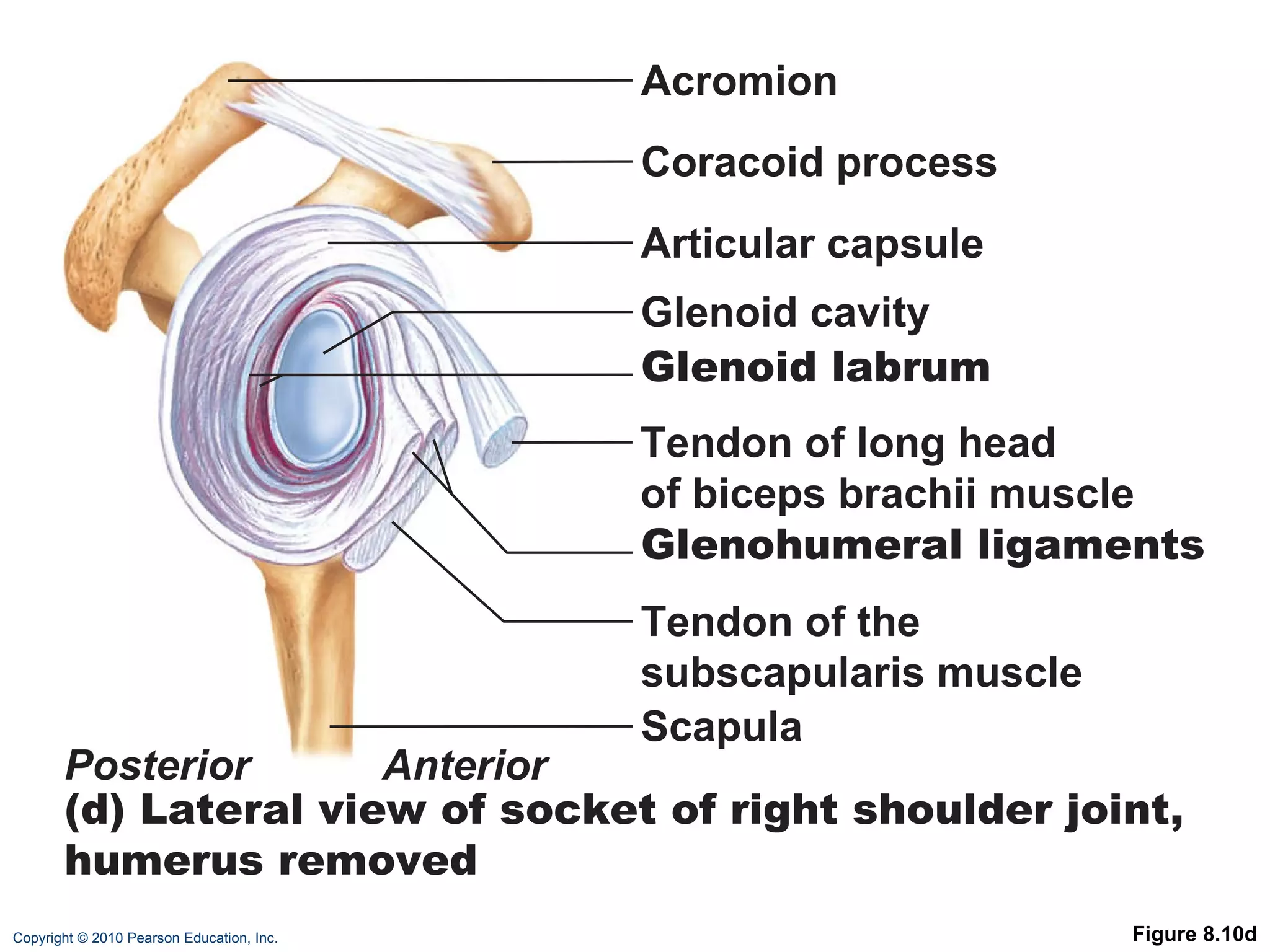
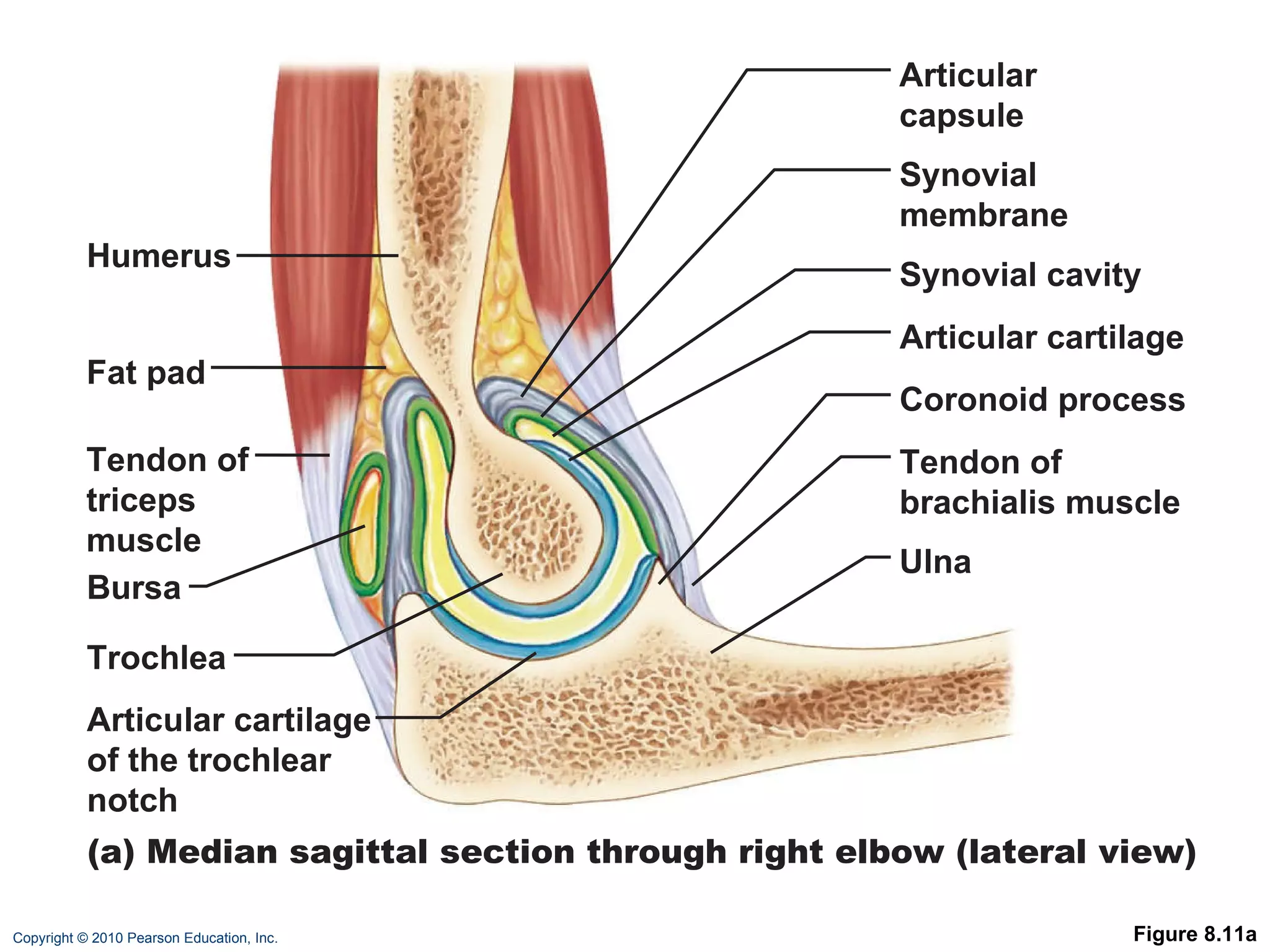
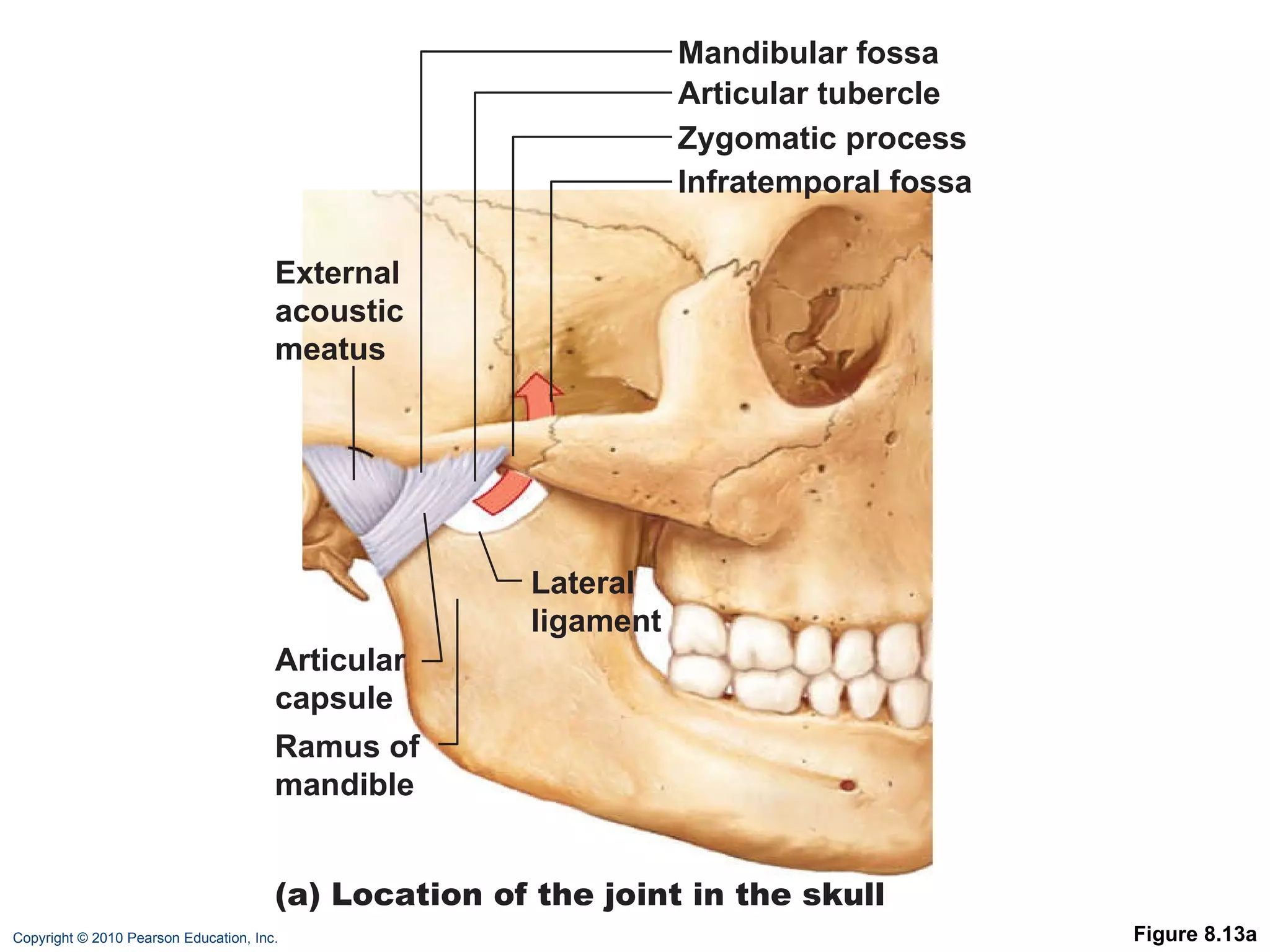
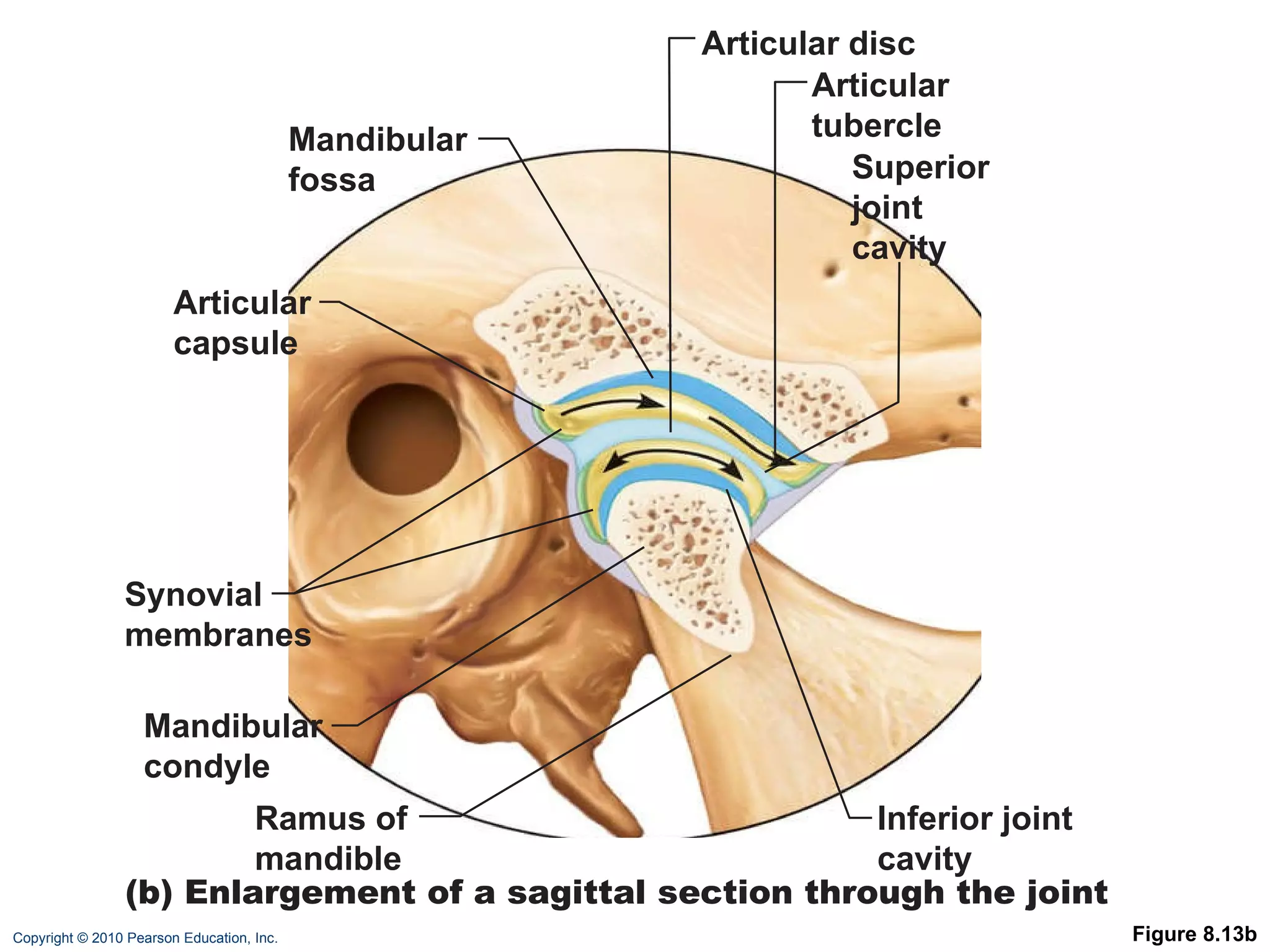
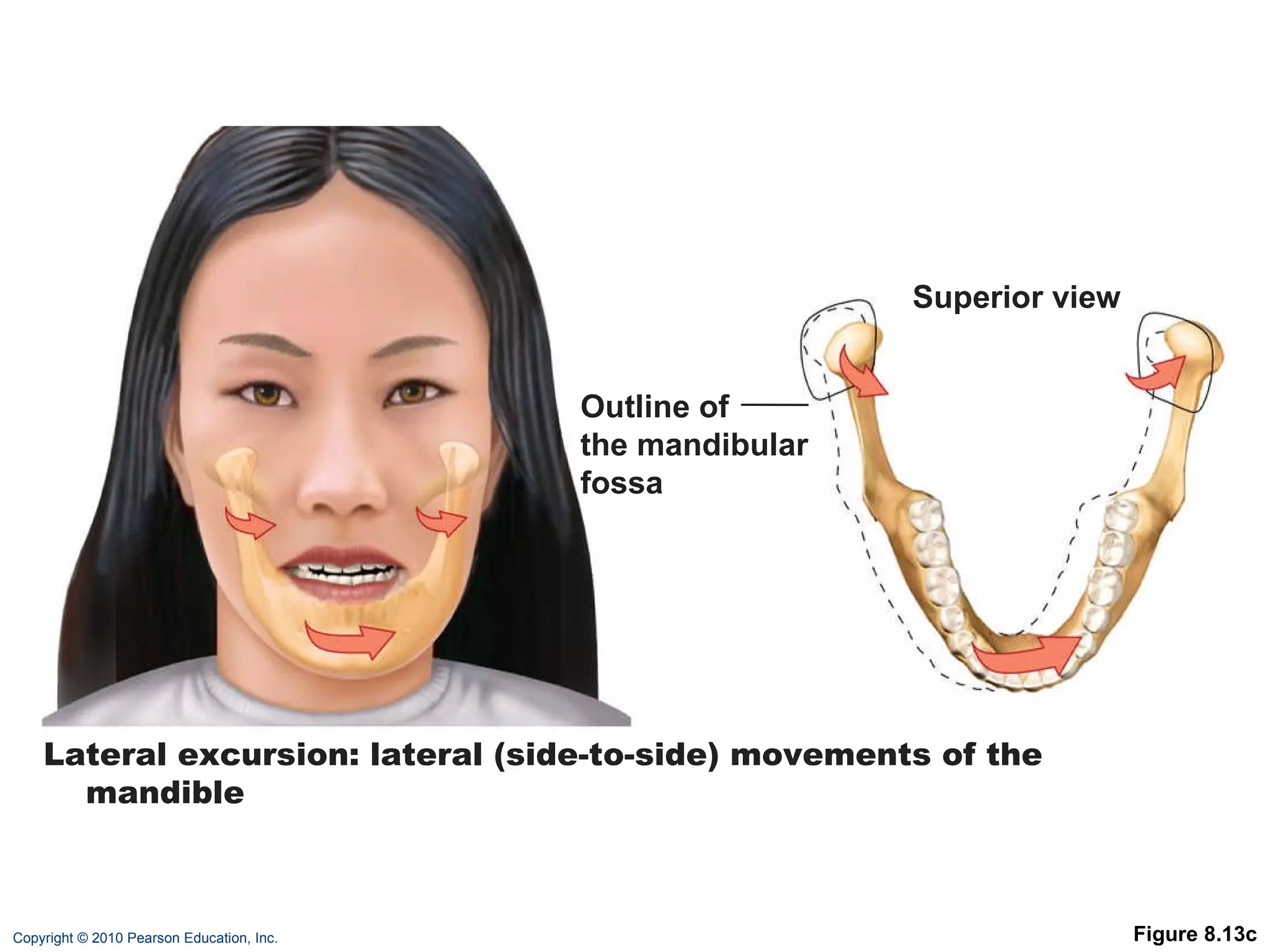
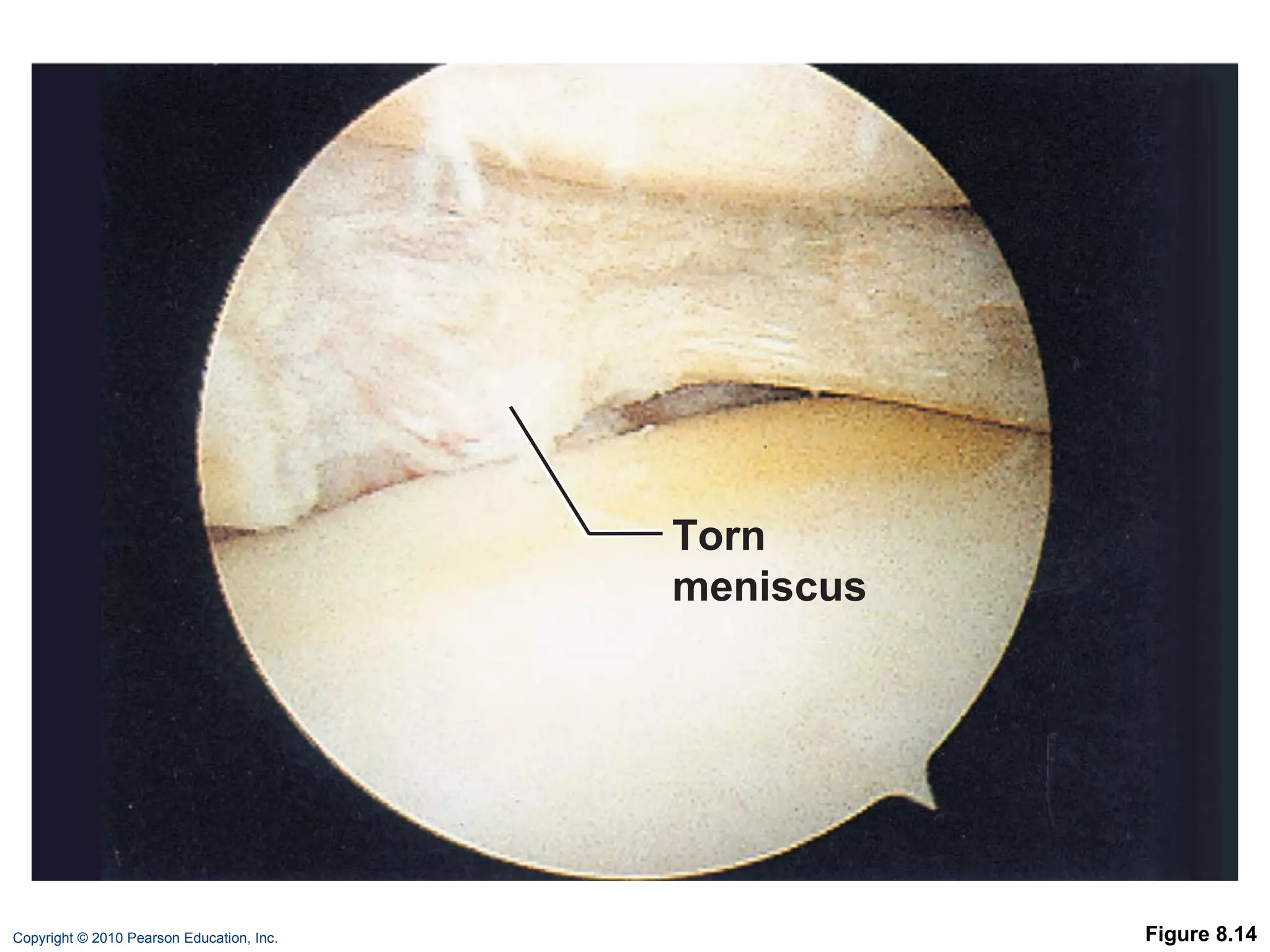
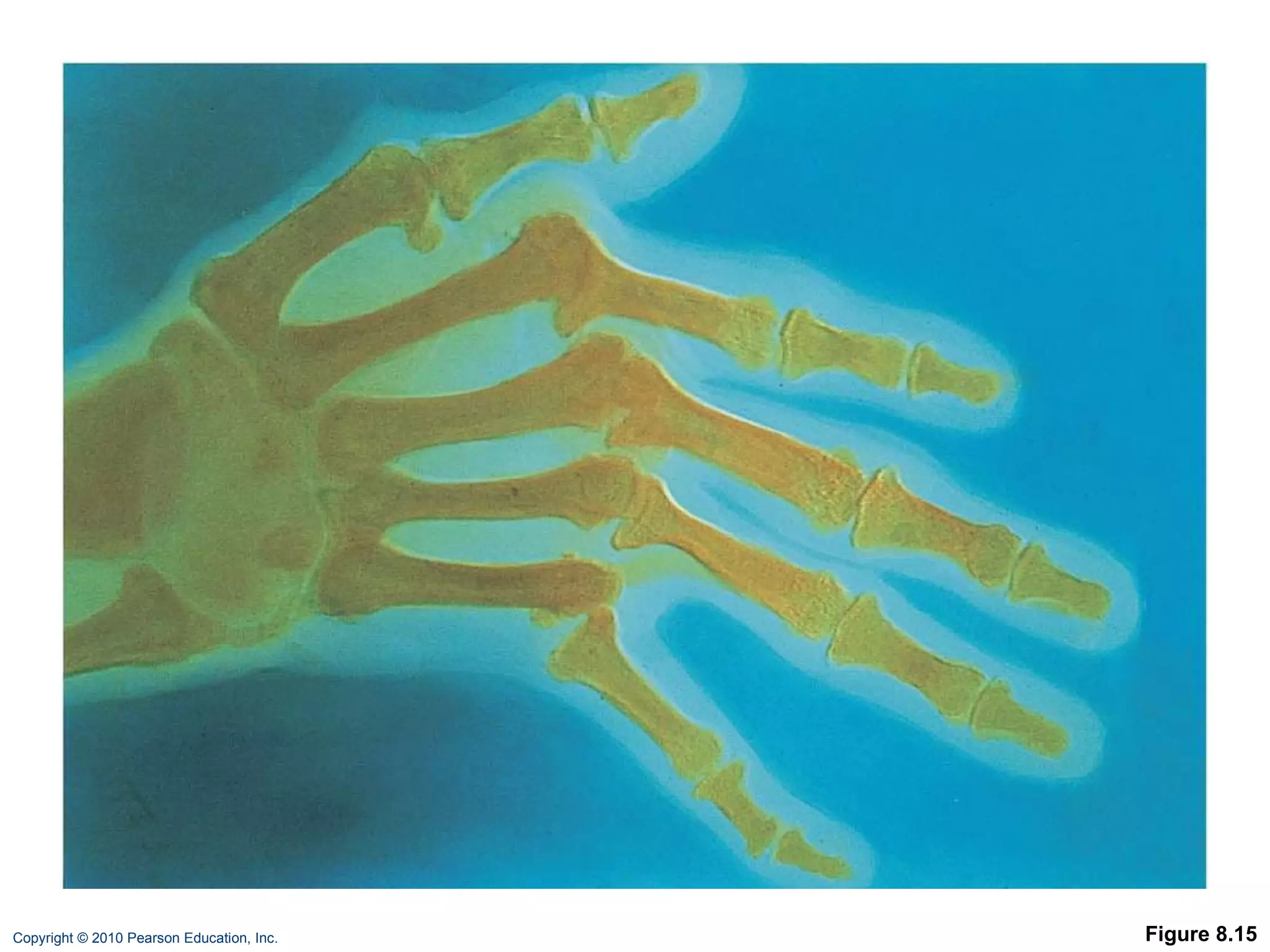
The document describes the six main types of synovial joints classified based on the shape of their articular surfaces: plane, hinge, pivot, condyloid, saddle, and ball-and-socket joints. It then provides more details on specific joints like the knee, shoulder, elbow, hip, temporomandibular, and common joint injuries and conditions like arthritis.



















































![Chapt08 Holes Lecture[1]](https://cdn.slidesharecdn.com/ss_thumbnails/chapt08holeslecture1-091122122447-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

























