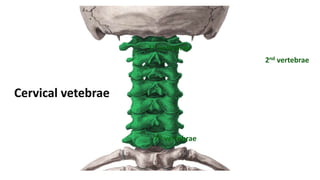
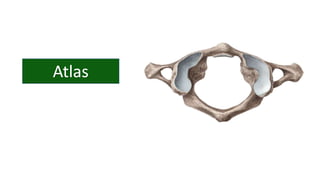
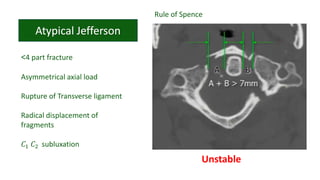
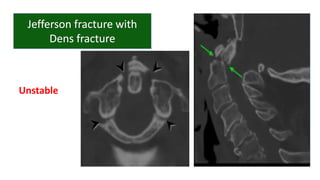
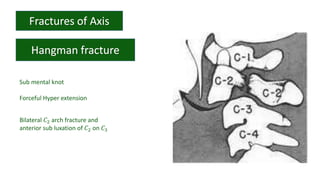
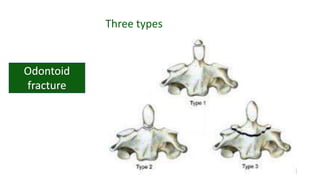
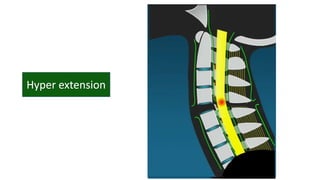
This document discusses cervical spine pathology and injuries. It covers the anatomy of the cervical vertebrae and joints. It then describes three common types of cervical spine injuries: fractures, subluxations, and dislocations. It notes how the mechanism of injury relates to whether the injury is stable or unstable. Key cervical injuries mentioned include odontoid fractures, facet dislocations, and atlanto-occipital dislocations.
































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







